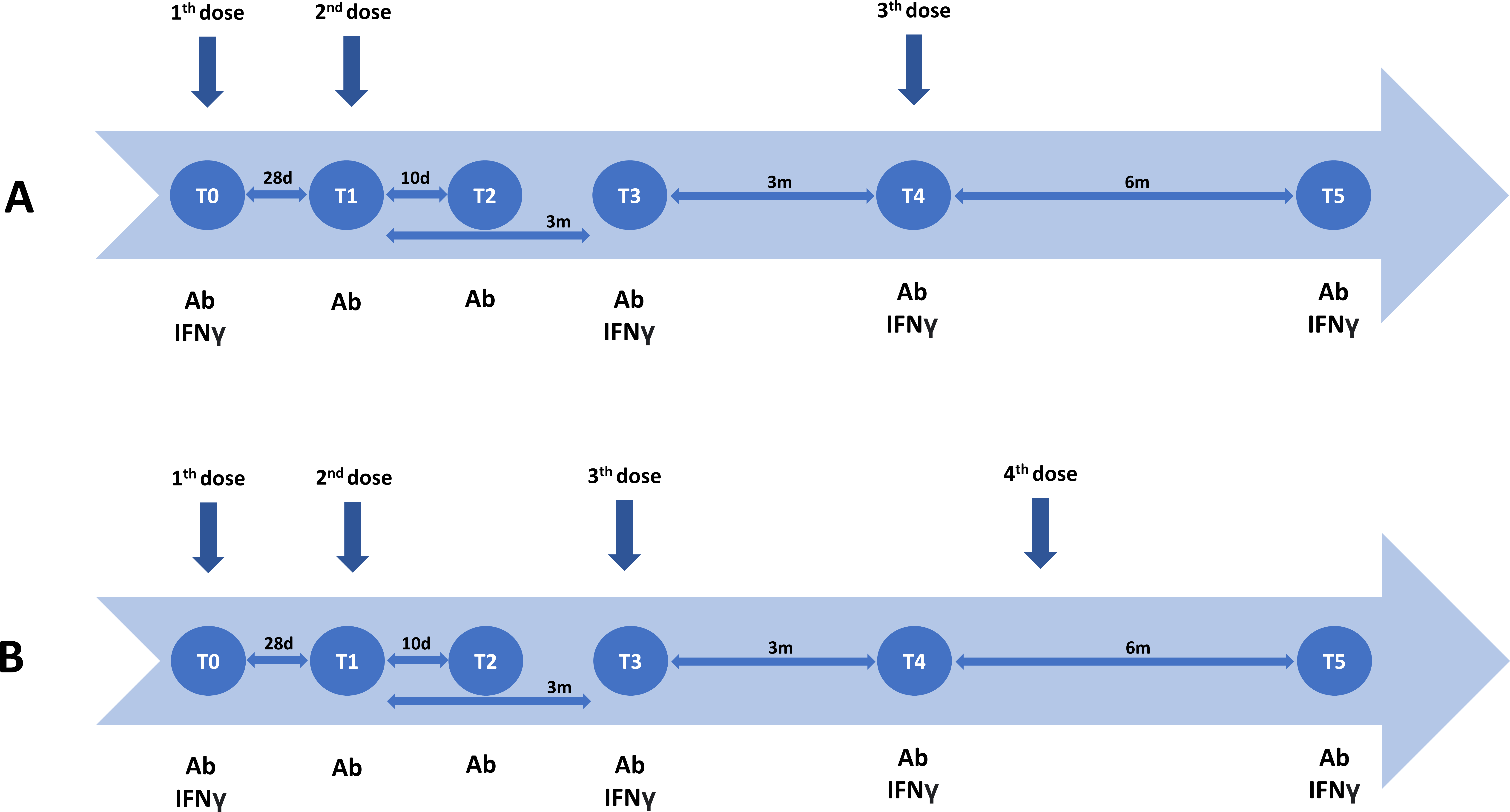
Background Immunocompromised patients are at risk for more severe COVID-19 infection and may have lower vaccination efficiency. In this report, we evaluate immunogenicity one year after standard regimen of mRNA vaccine administration in cohorts of primary or secondary immunocompromised patients. Methods In line with National recommendations, a third and fourth dose of the BNT162b2 (BioNTech) was administered to five clinical groups of immunocompromised patients, including primary immunodeficiency (PID) (n=57), people living with HIV (PLWH) (n=27), secondary immunocompromised patients with a broad variety of underlying rheumatologic (n=23) and homogeneous (multiple sclerosis) neurologic (n=53) conditions and chronic kidney disease (CKD) (n=39)] patients as well as a healthy control group (n=54). Humoral and cellular immune responses were evaluated at pre-defined time-points up to one year after standard vaccination. Results All PLWH and CKD patients and almost all (98.2%) of the PID patients had measurable antibodies 3 and 6 months after administration of the third and fourth vaccine dose. In contrast, 53.3% and 83.3% of the neurologic and rheumatologic patients, respectively, developed a humoral immune response after a third and fourth vaccine dose. In contrast to the other patient groups, all PLWH developed a cellular immune response after administration of 4 vaccine doses. In addition, cellular immune response was positive in 89.6%, 97.8%, 73.3% and 96.9% of the PID, neurologic, rheumatologic and CKD patients, respectively. Unlike the other groups, only the neurologic patient had a significantly higher cellular immune response compared to the healthy control group. Depending on the time point and epitopes used for cell stimulation, significant correlations between the humoral and cellular immune responses were observed in all patient groups, except for the neurology patient group. Conclusion Administration of a third and fourth vaccine dose results in retained or increased humoral and cellular immune response in patients with acquired or inherited immune disorders. The underlying condition, immunosuppressive treatment and/or individual risk factors may explain delayed humoral, cellular or both immune responses.