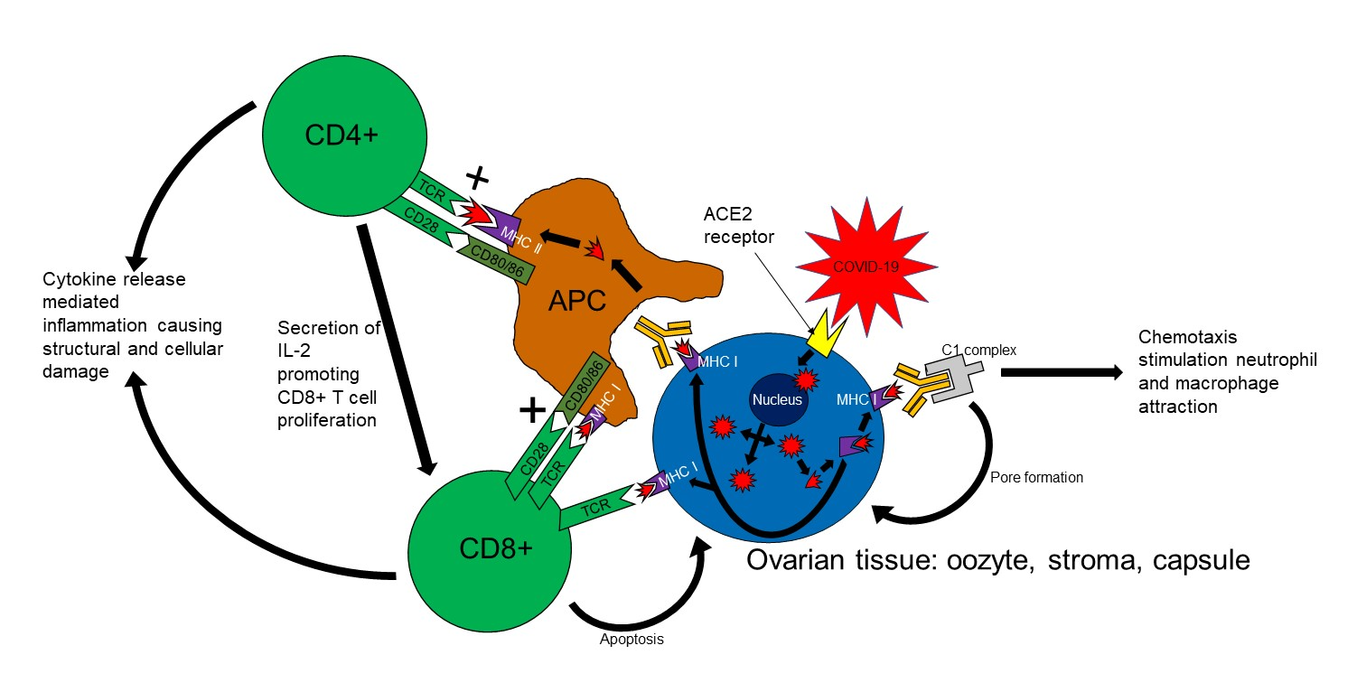
Premature ovarian insufficiencysecondary to COVID-19 infection: an original case reportShortened title: COVID-19 induced premature ovarian insufficiencyDr James Wilkins1Email address: [email protected]: +447564 977847Address: Department of Obstetrics and GynaecologySouth Tyneside & Sunderland Royal HospitalSouth ShieldsNE34 0PL United KingdomDr Shamma Al-Inizi2Email address: [email protected]: +447821 708743Address: Department of Obstetrics and GynaecologySouth Tyneside & Sunderland Royal HospitalSouth ShieldsNE34 0PL United Kingdom1 Foundation doctor in the department of Obstetrics and Gynaecology, South Tyneside & Sunderland NHS Foundation Trust, United Kingdom2 Consultant Obstetrician and Gynaecologist, Department of Obstetrics and Gynaecology, South Tyneside & Sunderland NHS Foundation Trust, United KingdomMain DocumentBackground:In late December 2019, several patients began to develop signs and symptoms consistent with a viral pneumonia in Wuhan, China. This disease spread, becoming a global pandemic and was eventually identified to be a novel strain of coronavirus termed coronavirus disease 2019 (COVID-19). A significant proportion of patients infected with this virus unfortunately develop severe disease associated with acute respiratory distress syndrome, hypercoagulability and neurological disease amongst other complications(1) and, as of the 16/2/21, there have been 108.7 million cases and 2.4 million reported deaths globally(2). There is increasing recognition that a proportion of patients who contract this acute infection will develop a subsequent long-term illness. The range of symptoms attributed to this is large but most commonly include fatigue, shortness of breath and myalgia(3). This long-term illness is thought to be secondary to chronic tissue inflammation. There is a risk that reproductive tissue may also be vulnerable, potentially resulting in subfertility, but to date no cases of deranged ovarian function secondary to COVID-19 have been reported.Case report:A 34-year-old lady presented to the fertility clinic at South Tyneside District Hospital in November 2020 with primary subfertility after having regular unprotected sexual intercourse for over one year. She and her partner were investigated for this; a hysterosalpingogram demonstrated patent fallopian tubes and her partner’s seminal fluid analysis was normal. Ovarian function was investigated with blood tests. These demonstrated high gonadotrophin levels and a very low progesterone level of 0.3nmol/L consistent with premature ovarian insufficiency (POI). The common causes of this were investigated but none were identified, nor did she have a positive family history of POI. Polycystic ovarian syndrome was excluded due to a normal transvaginal ultrasound scan and lack of clinical and biochemical evidence of hyperandrogenism. She was a non-smoker with a healthy BMI, had had neither pelvic surgery nor chemo/radiotherapy previously. In terms of comorbidities, she was fit and well other than well controlled hypothyroidism, which was medicated with levothyroxine with a recent TSH of 0.98mUI/L, in the normal range.Interestingly, this lady was diagnosed with COVID-19 in April 2020 by a nasopharyngeal swab demonstrating positive viral serology. During the acute illness she developed symptoms of shortness of breath, fatigue, myalgia and headache but did not require hospitalisation nor active treatment for these symptoms. Her shortness of breath improved over the course of two to three weeks but she experienced persistent fatigue and continuing myalgia over the next few months. She has been referred to the long COVID clinic due to this. In addition, her periods became irregular with oligomenorrhoea and she began to experience regular hot flushes and night sweats. Two months prior to contracting COVID-19, in February 2020, she was referred to the fertility clinic and at this time she had normal regular periods and normal gonadotrophin levels: FSH 8U/L and LH 2U/L. However in November 2020, seven months after her acute infection, her FSH was 78U/L and LH 43U/L and on repeat two months later her gonadotrophins were persistently raised: FSH 89U/L and LH 32U/L.These events mean that this lady is very unlikely to fall pregnant without support and one of the available options is trying to conceive via assisted reproduction with egg donation or adoption, hence a referral to the local IVF centre was arranged.Due to the novel nature of this presentation, written consent to publish this case was obtained from the patient.Discussion:It is well established that viruses can cause inflammation of reproductive tissue; indeed one of the most common clinical manifestations of mumps is orchitis, which can be damaging to testicular function. Further, several case reports have discussed the development of orchitis in patients who have contracted COVID-19 and small studies have shown pathological changes to testicular tissue in some affected with this virus(4). A possible mechanism for this is expressed in Figure 1. Reproductive tissue expresses the ACE2 receptor and COVID-19 may utilise this to gain cellular entry(5, 6). Viral entry to these cells would promote an inflammatory response through the complement cascade and associated chemotaxis, phagocytosis of virally infected cells and presentation of this antigen causing local T cell activation and cytokine release by a myriad of immunological cells(7). These effects have the potential to cause significant cellular demise either directly through apoptosis and phagocytosis or indirectly through mechanisms such as the disruption of tissue microvasculature(7). These could cause sufficient damage to impair steroidogenesis and ovulation affecting fertility.Despite this mechanism and positive histological findings in males, to date these studies have not found these microscopic changes in ovarian tissue following infection with COVID-19 nor have there been case reports describing an effect of COVID-19 on female sex hormones or fertility. This may be due to several factors. Firstly, the ACE2 receptor is less expressed in ovarian tissue compared to testicular tissue(8) meaning the change of viral invasion to this tissue and subsequent damage may be less. Another explanation may be that there have been very few studies examining ovarian tissue histologically following COVID-19. This means it is very possible an effect of COVID-19 on this tissue may have thus far gone undetected. In addition, investigation of subfertility is normally only undertaken following a minimum of one year of regular unprotected sex. As the pandemic began to spread worldwide in early 2020, it is likely that if COVID-19 were to impact on the ovarian function of a significant proportion of women then the impact of this would not be investigated until early 2021 and therefore would not begin to be apparent until this time.The COVID-19 pandemic is the largest health challenge the world has faced in modern times with many people already having been infected by this virus. The possibility that a cohort of women may have contracted thus far undiagnosed COVID-19-induced subfertility with more at risk of developing this, means that health professionals working in fertility should be highly alert to this potentiality and more work should be performed to investigate this further. If more evidence is gathered consistent with this hypothesis, then a lower threshold for treatment aiming to reduce inflammation to protect ovarian function should be considered and women should be made aware of this risk.Word count: 1025 words.DeclarationsWe have no conflicts of interest related to this publication to declare and there has been no financial support for this work. The finished publication has been reviewed and approved for submission by all corresponding authors. Written consent for this case report has been obtained from the patient and as this work is a case report formal ethical approval was not required.Contribution to authorshipPrimary Author: Dr James Wilkins (JW)JW assessed the patient about whom this case report is detailed in clinic alongside SAI and, following this, planned this case report, assessed the background literature and hypothesised a potential mechanism for the association described. Following this, JW wrote up this work with contributions from SAI.Secondary Author: Dr Shamma Al-Inizi (SAI)SAI was the primary assessor of this lady in her subfertility clinic and suggested the case would merit publication, encouraging JW with this. SAI then reviewed the work produced by JW making changes and suggestions as appropriate in the writing up process before giving her approval for submission.Figures:Figure 1: Possible mechanism of COVID-19 induced premature ovarian insufficiencyReferences:1. Public Health England. COVID-19: epidemiology, virology and clinical features. 2021.2. World Health Organisation. Coronavirus disease (COVID-19) pandemic, Available at: .3. Iacobucci G. Long covid: Damage to multiple organs presents in young, low risk patients. BMJ. 2020;371:m4470.4. Madjunkov M, Dviri M, Librach C. A comprehensive review of the impact of COVID-19 on human reproductive biology, assisted reproduction care and pregnancy: a Canadian perspective. Journal of Ovarian Research. 2020;13(1):140.5. Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020;181(2):271-80.e8.6. Henarejos-Castillo I, Sebastian-Leon P, Devesa-Peiro A, Pellicer A, Diaz-Gimeno P. SARS-CoV-2 infection risk assessment in the endometrium: viral infection-related gene expression across the menstrual cycle. Fertil Steril. 2020;114(2):223-32.7. Murphy K, Weaver C. Janeway’s Immunobiology. 9 ed: W. W. Norton & Company; 2017 2017. 928 p.8. Hikmet F, Méar L, Edvinsson Å, Micke P, Uhlén M, Lindskog C. The protein expression profile of ACE2 in human tissues. Molecular Systems Biology. 2020;16(7):e9610.