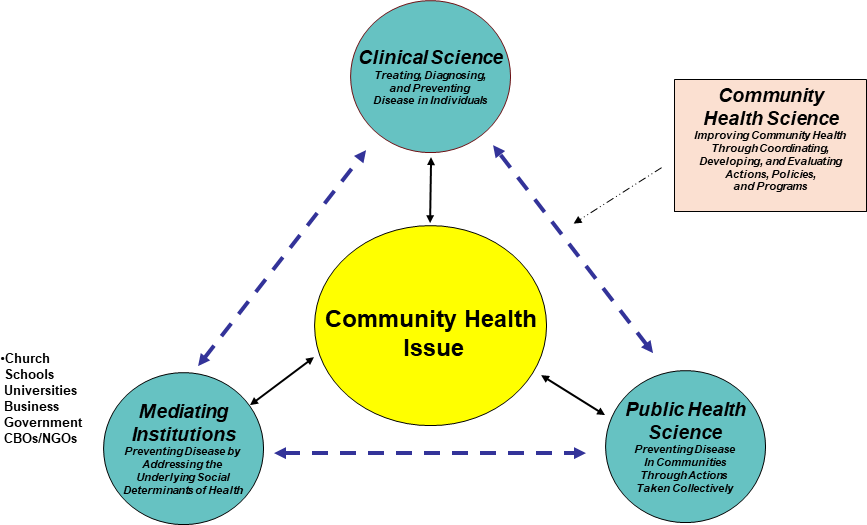
In the United States chronic illnesses have become a way of life for multiple generations – they are the number one cause of death and disability (accounting for more than 70% of deaths), 60% of American adults have at least one chronic disease, and 40% have multiple chronic conditions. Although multiple factors contribute to the growth in chronic disease prevalence, a major factor has been overreliance on health care systems for promoting health and preventing disease. Large health care systems are ill equipped for this role since they are designed to detect, treat, and manage disease, not to promote health or address the underlying causes of disease. Improving health outcomes in the U.S. will require implementing broad-based prevention strategies combining biological, behavioral, and societal variables that move beyond clinical care. According to community medicine, clinical care alone cannot create, support, or maintain health. Rather, health can only ensue from combining clinical care with epidemiology and community organization, because health is a social outcome resulting from a combination of clinical science, collective responsibility, and informed social action. During the past 20 years, our team has developed an operational community medicine approach known as community health science. Our model provides a simple framework for integrating clinical care, population health, and community organization, using community-based participatory research (CBPR) practices for developing place-based initiatives. In the present paper, we present a brief overview of the model and describe its evolution, applications, and outcomes in two major urban environments. The paper demonstrates means for integrating the social determinants of health into collaborative place-based approaches, for aligning community assets and reducing health disparities. We conclude by discussing how asset-based community development can promote social connectivity and improve health, and discuss how our approach reflects the emerging national consensus on the importance of place-based population system change.