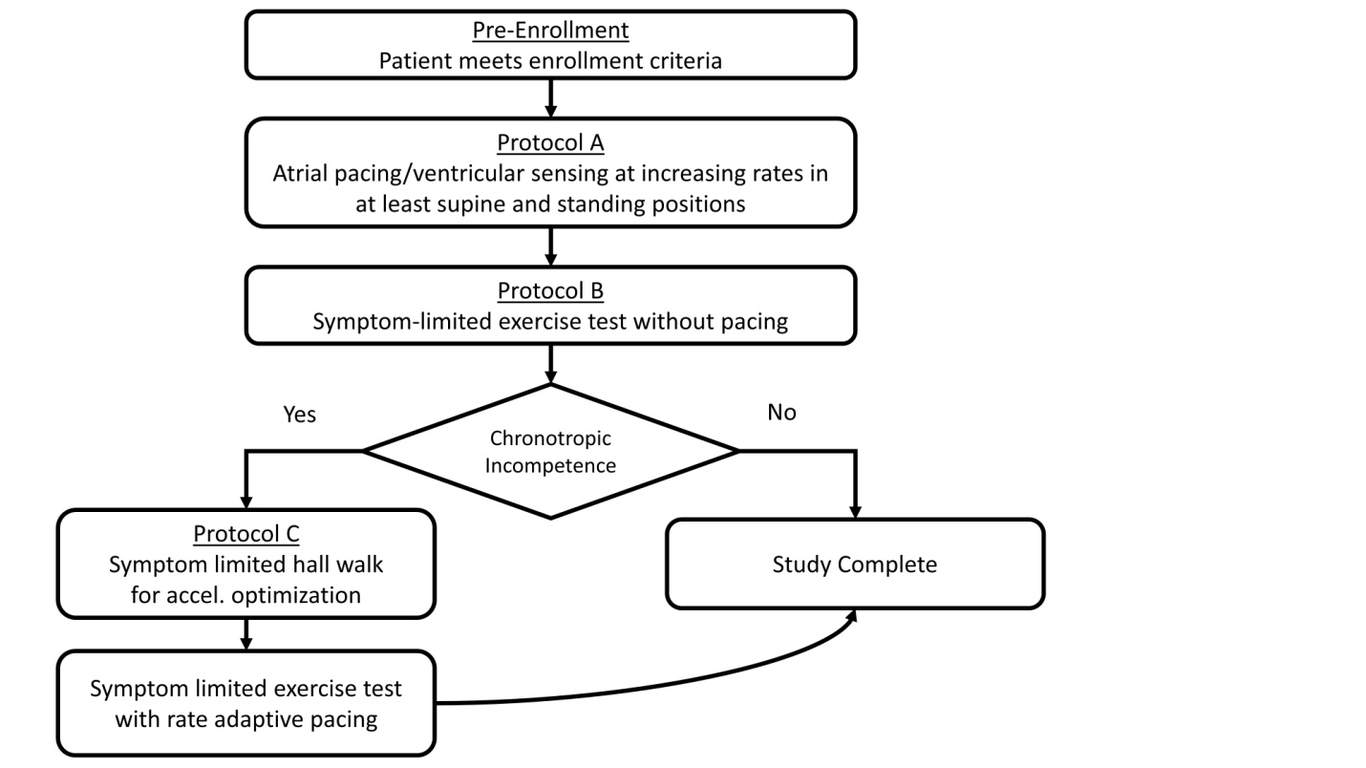
Objectives: To evaluate changes in intrinsic atrioventricular (AV) conduction associated with exercise and atrial pacing among heart failure patients with cardiac resynchronization therapy (CRT). Methods: RAVE was a multicenter prospective trial of CRT patients. Heart rate was increased with incremental atrial pacing up to 130 beats/min and with submaximal exercise without atrial pacing. According to maximal heart rate achieved during exercise, patients whose maximal heart rate < 100 bpm or 75% of 85% of age predicted max heart rate were diagnosed with chronotropic incompentence(CI). Others were classified as patients with chronotropic compentence(CC). For CI patients, an additional symptom limited exercise with rate adaptive pacing activated was performed. Intracardiac intervals were measured from the implantable lead electrograms. Results: There were 12 subjects with CI and 24 with CC. With atrial pacing, AV interval immediately increased and gradually increased with incremental atrial pacing in all patients. However, the changes in the atrial to right ventricular (ARV) and atrial to left ventricular (ALV) intervals with increasing atrial pacing rates were about 3-fold greater in CI patients compared to CC patients (28.3±29.5 vs. 10.8±8.9 ms/10 bpm for ARV and 25.5±22.1 vs. 9.9±8.8 ms/10 bpm for ALV in the supine position, p < 0.05). In CI pacing with rate-adaptive pacing during exercise, AV interval changes with paced heart rate were variable. Conclusions: AV response to overdrive atrial pacing at rest may provide a simple means of identifying chronotropic competence in CRT patients. For patients with CI, who often require rate-adaptive atrial pacing, rate-adaptive AV algorithms should be adjusted individually.