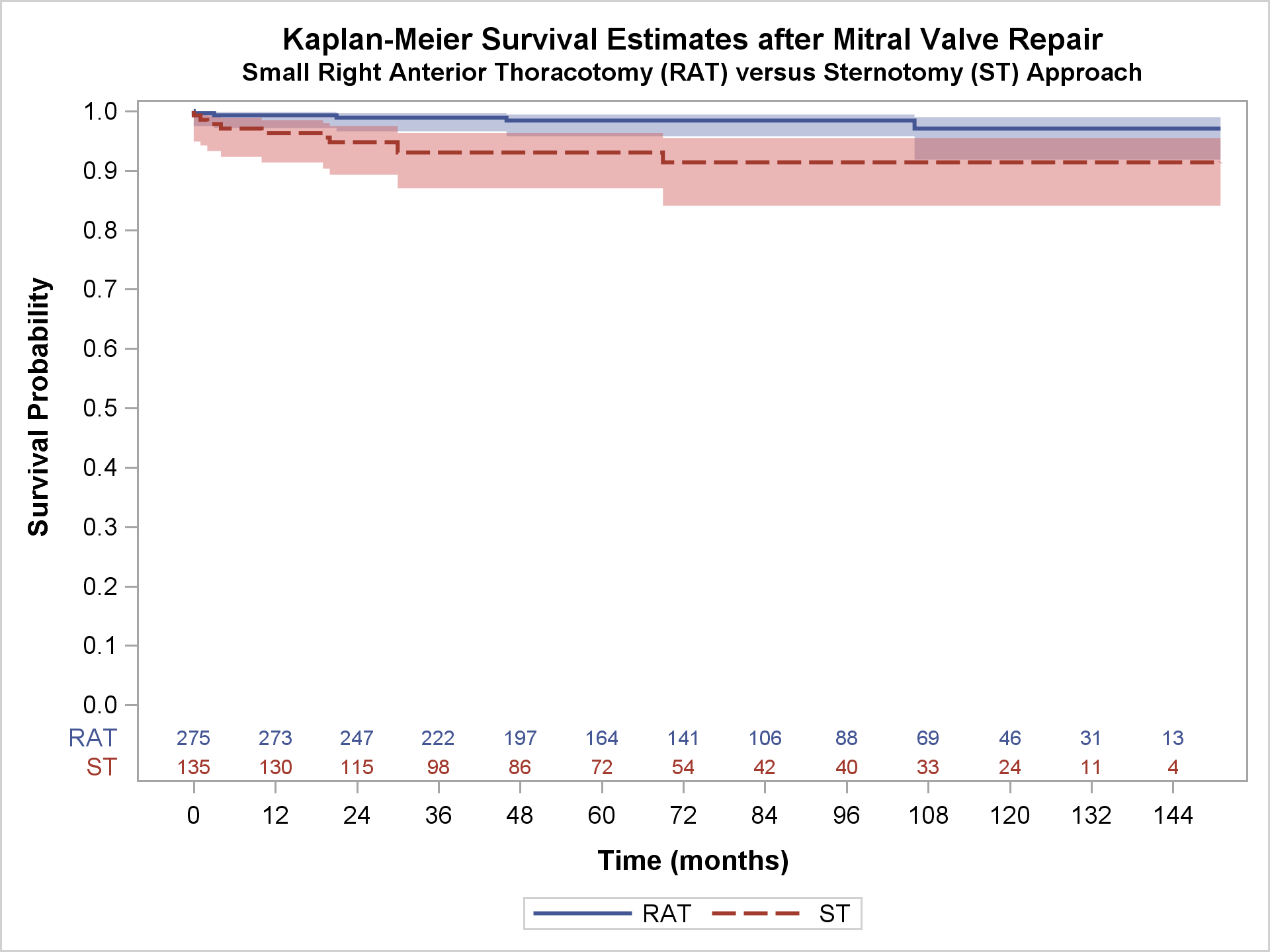
Background: Controversy exists regarding durability and survival after mitral valve repair between sternotomy and a small right anterior thoracotomy approaches. Methods: Between February 2004 and July 2015, 410 patients underwent mitral valve repair via either sternotomy (ST, n=135) or small right anterior thoracotomy (RAT, n=275). Mean follow up was 72.7 38.9 months. Postoperative echocardiograms were obtained in 310 patients (75.6%) at a mean of 20.3 21.4 months. Results: Overall survival at 1, 3, 5, and 10 years were 96.3, 93.0, 93.0, and 91.4% for the ST group and 99.3, 98.9, 98.4, and 97.0% for the RAT group (Log-Rank p = 0.004). There was no difference between groups in the cumulative incidence of need for mitral valve reoperation or progression of mitral regurgitation (MR) considering death as a competing outcome over time (p=0.94 and 0.53, respectively). Propensity score weighted multivariate Cox Proportional hazard modeling built on baseline differences between the RAT and ST groups, showed presence or absence of posterior or anterior leaflet pathology was not associated with mortality, need for reoperation, or progression of MR. A RAT approach was associated with a decreased mortality on adjusted analysis (hazard ratio, 0.32, 95% confidence interval, 0.13-0.82, p=0.018), however, this result was less significant when those with coronary artery disease were removed (hazard ratio, 0.34, 95% confidence interval, 0.12-0.96, p=0.041). Conclusions: Mitral valve repair via a small right anterior thoracotomy incision in select patients can be performed with surgical results and survival that are equivalent to the sternotomy approach.