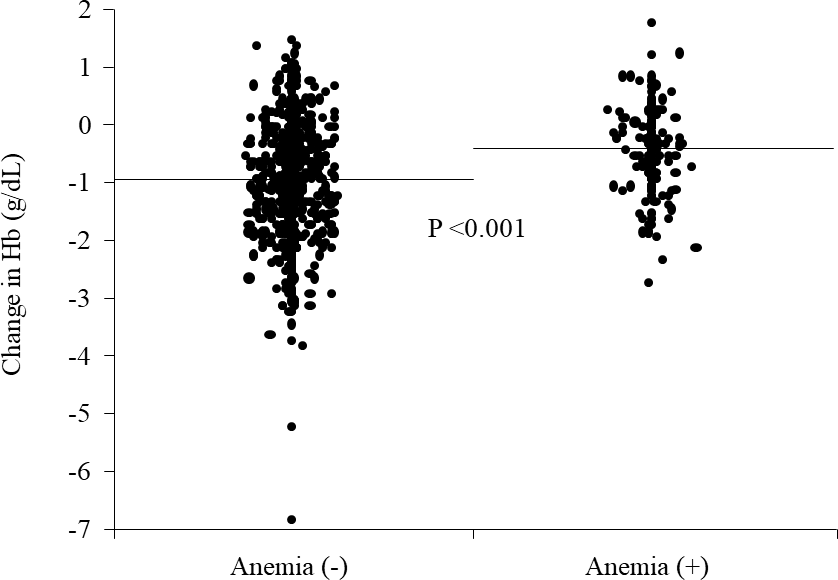
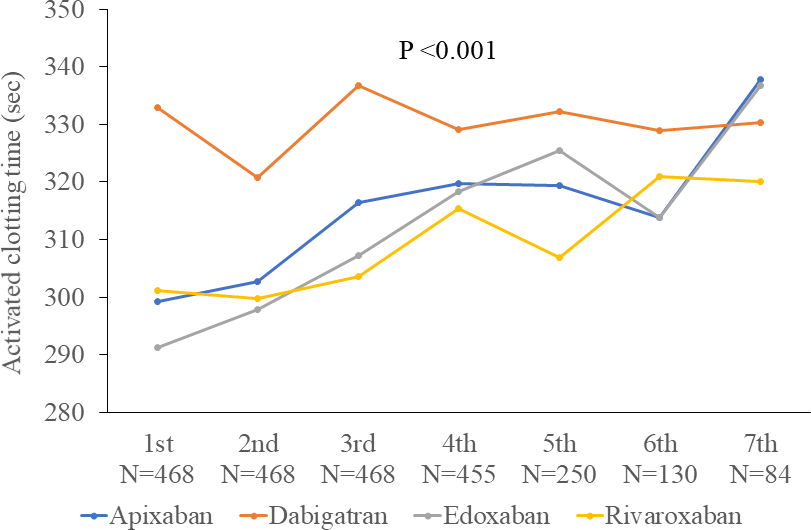
Background: Thromboembolic or hemorrhagic complications related to atrial fibrillation (AF) ablation are rare, and thus, it is difficult to compare their frequency across different direct oral anticoagulants (DOACs). We aimed to compare the intraablation blood coagulability and postprocedural hemoglobin fall as alternatives to those complications across 4 DOACs. Methods: We enrolled AF patients younger than 65 years old in 3 cardiovascular centers who skipped a single dose of apixaban, dabigatran, edoxaban, and rivaroxaban, prior to the ablation. Endpoints included the activated clotting time (ACT), heparin requirement during the ablation, and drop in the hemoglobin level 24 hours after the procedure. Results: The time-course curves of the ACT differed significantly across the patients with apixaban (N=113), dabigatran (N=130), edoxaban (N=144), and rivaroxaban (N=81), with its highest level in the dabigatran group (P <0.001). The average ACT was greater in the dabigatran group than in the other groups (312.3±34, 334.4±44, 308.1±41, and 305.8±34.7 sec; P <0.001). A significant difference was noted in total heparin requirement across the patient groups (3990.2±1167.9, 3890.4±955.3, 4423.8±1051.6, and 3972±978.7 U/m2/h; P <0.001), with its greatest amount in the edoxaban group. The reduction in the hemoglobin level was similar (-0.93±0.92, -0.88±0.79, -0.89±0.97, -0.95±1.23 g/dL; P=0.94). No inter-group difference was noted in the rate of major or minor bleedings (0.9%, 2.3%, 1.4%, and 3.7%; P=0.51), and no thromboembolic events were encountered. Conclusion: A difference in DOACs may have an impact on intraablation anticoagulation, however, it may not on the procedural blood loss in the setting of a single skip.