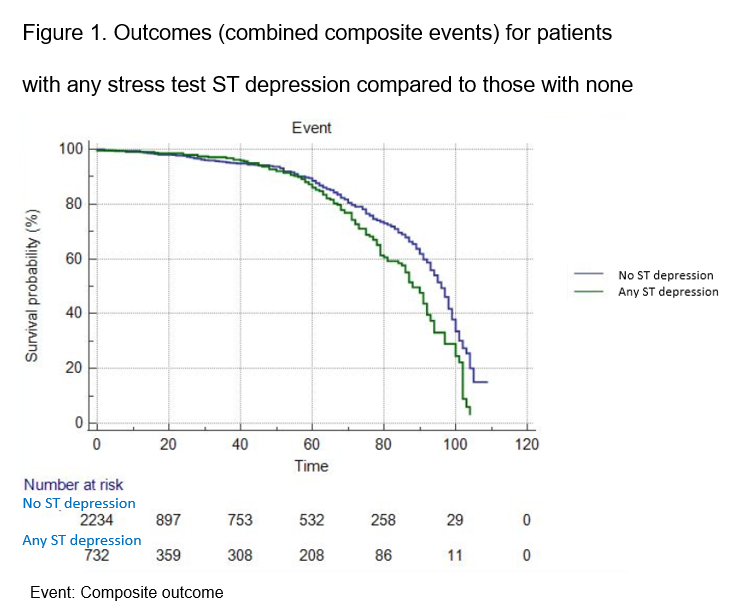
Background. Electrocardiographic (ECG) changes during stress testing are a common and perplexing finding during non-ischaemic stress echocardiography (SE). Research has provided conflicting results regarding the implications. Methods. SE was performed after maximal Bruce protocol treadmill exercise. Results. 3020 consecutive patients, mean age 58±12 years, 36% female, were followed-up for up to 9 years (mean 36±21 months) post SE. Time to first cardiac event (composite of heart failure admission, worsening New York Heart Association class, worsening ejection fraction, acute coronary syndrome, revascularization, angina or cardiovascular death) was analyzed and adjusted using Cox proportional hazards regression. Prognostic significance was found with 1.5mm of downsloping or horizontal ST depression. Adjusting for baseline differences, increased risk of composite major adverse cardiac events was shown with at least 1.5mm of exercise induced ST depression (Hazard ratio [HR] of 2.47, 95% Confidence ratio [CI] 1.67-3.72, p<0.0001). Patients achieving high level exercise capacity (≥13 metabolic equivalents or METs) with ST depression lower risk of cardiac events during follow-up Conclusion. Patients with ST segment depression but non-ischaemic stress imaging have poorer prognosis compared to patients with non-ischaemic stress echocardiograms with normal stress ECGs. ST depression of 1.5mm or more was established as a prognostically significance value. High exercise capacity improves prognosis, and ECG changes in that setting can be regarded as false positives. Overall, however, ST depression during non-ischaemic stress imaging is not a benign finding.

/Figure 1 (1).png?1598712428)