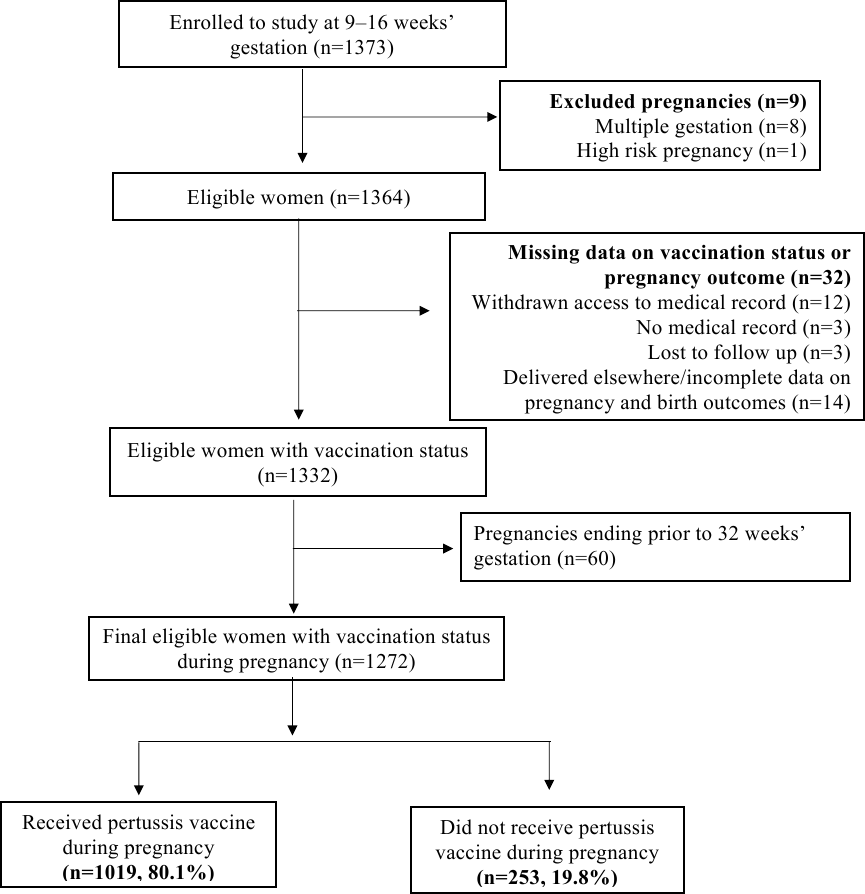
Abstract Objective To evaluate the safety of maternal pertussis vaccination on pregnancy and birth outcomes. Design Prospective, multicentre cohort study. Setting Two major materiality hospitals in South Australia. Population A total of 1364 low-risk nulliparous women with a singleton pregnancy recruited at 9–16 weeks’ gestation between 2015 to 2018. Methods Participants were followed prospectively, with vaccination (confirmed by medical records), extensive amounts of pregnancy and birth outcome data collected by research midwives. Adjusted relative risks (aRRs) and hazard ratios (aHRs) were estimated accounting for time-varying vaccine exposure and the temporal nature of each outcome. Main Outcome Measures Pregnancy and birth outcomes. Results Of the 1272 women included in this study, 80.1% (n=1019) received maternal pertussis vaccination. Vaccinated women had an average 0.22 weeks (95% CI 0.001, 0.44) longer gestation at delivery compared to unvaccinated women. Maternal pertussis vaccination was not associated with chorioamnionitis (aRR 0.71, 95% CI 0.27,1.82), gestational hypertension (aHR 1.24, 95% CI, 0.66, 2.30), preeclampsia (aHR 0.75, 95% CI 0.47, 1.18) nor preterm birth (aHR 0.99, 95% CI 0.47, 2.07). Neither risk of low birth weight (aHR 0.72, 95% CI 0.41, 1.27) nor small for gestational age infants (aHR 0.67,95% CI 0.29, 1.55) were increased following maternal pertussis vaccination. No associations between pertussis vaccination during pregnancy and adverse birth outcomes including admission to the neonatal care unit, low Apgar scores, and mechanical ventilation were observed. Conclusions Our study provides reassuring evidence of the safety of maternal pertussis vaccination with no increased risk of adverse pregnancy and birth outcomes.