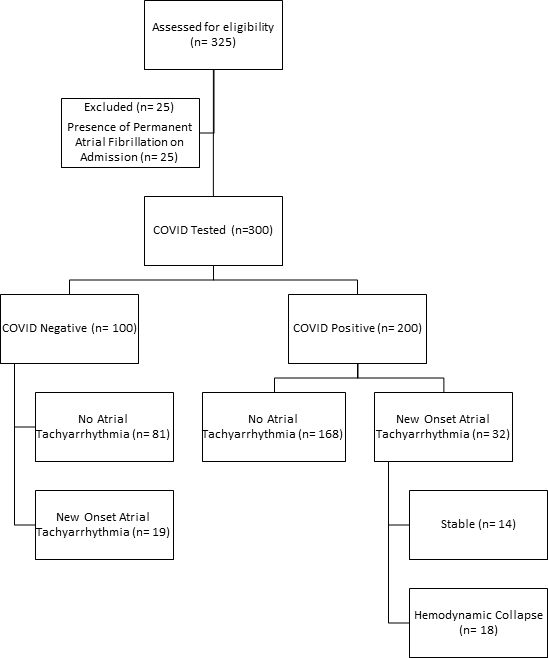
Rationale: Coronavirus Disease 2019 (COVID-19) is associated with many clinical manifestations including respiratory failure and cardiovascular compromise.Objectives: We examine outcomes in critically ill individuals with COVID-19 who develop atrial tachyarrhythmias.Methods: We collected data from electrocardiograms and the electronic medical record of COVID-19 positive (COVID+) and negative (COVID-) individuals admitted to our medical intensive care unit between February 29 and June 28, 2020. We compared clinical and demographic characteristics, new onset atrial tachyarrhythmia, hemodynamic compromise following atrial tachyarrhythmia, and in-hospital mortality in COVID+ vs. COVID-. Hemodynamic compromise was defined as having a new or increased vasopressor requirement or the need for direct current cardioversion for hemodynamic instability within 1 hour of atrial tachyarrhythmia onset.Results: Of 300 individuals included, 200 were COVID+ and 100 were COVID-. Mean age was 60±16 years, 180 (60%) were males, and 170 (57%) were African American. New onset atrial tachyarrhythmia occurred in 16% of COVID+ and 19% of COVID- individuals (p=0.51). When compared to COVID- participants without atrial tachyarrhythmia, COVID+ individuals with new onset atrial tachyarrhythmia had higher mortality after multivariable adjustment (OR 5.0, 95% CI 1.9-13.5). New onset atrial tachyarrhythmia was followed by hemodynamic compromise in 18 COVID+ but no COVID- participants (P=0.0001). COVID+ individuals with hemodynamic compromise after atrial tachyarrhythmia required increased ventilatory support at the time of atrial tachyarrhythmia onset.Conclusions: Atrial tachyarrhythmia is associated with increased mortality in critically ill individuals with COVID-19, especially those mechanically ventilated. Recognition of this could assist with clinical care for individuals with COVID-19.