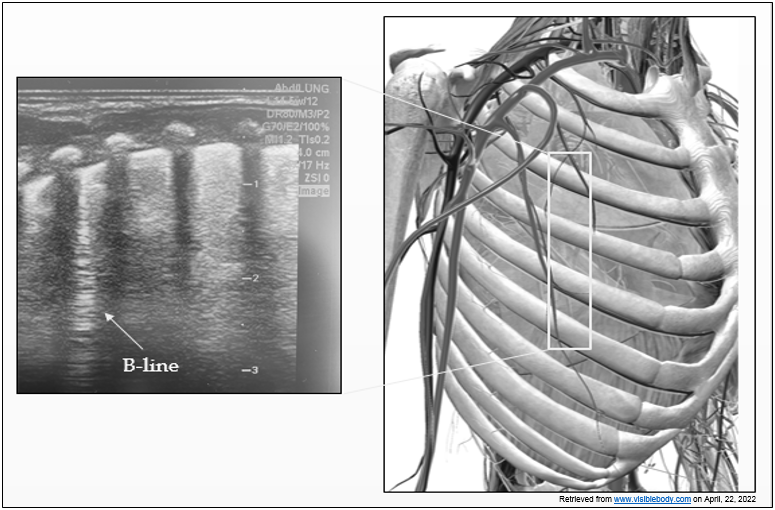
Introduction: Bronchopulmonary dysplasia (BPD) is characterized by lung injury with varying degrees of disrupted alveolarization, vascular remodeling, inflammatory cell proliferation, and pulmonary edema. Diuretics are often used to ameliorate the symptoms or progression of BPD. Our primary objective was to use lung ultrasound (LUS) to determine if diuretics decrease pulmonary edema in infants with BPD. The secondary objective was to assess changes in respiratory support during the first week after initiation of diuretics. Methods: Premature infants requiring non-invasive respiratory support and starting diuretic therapy for evolving BPD were compared with a similar group of infants not receiving diuretics (control). For the diuretic group, LUS exams were performed before and on days 1, 3 and 6 after initiation of treatment. For the control group, LUS was performed at equivalent time points. A composite pulmonary edema severity (PES) score of 0 to 5 was calculated based on the total number of B-lines in 6 scanned areas. Respiratory support parameters (FiO2, nasal cannula flow or CPAP) were also recorded. Results: Infants in the diuretic (n=28) and control (n=23) groups were recruited at median corrected gestational ages of 34.2 (33.3-35.9) and 34.0 (33.4-36.3) weeks, respectively ( p=0.82). PES scores, FiO2, and respiratory flow support decreased significantly from day 0 to 6 ( p<.0001, p=0.001, and p=0.01, respectively) in the diuretic group, but not in the control group. Conclusion: Diuretic use is associated with decreased pulmonary edema and improved oxygenation in infants with BPD during the first week of treatment.

/FIGURE 1 for PP SUBMISSION (4).png?1610380927)