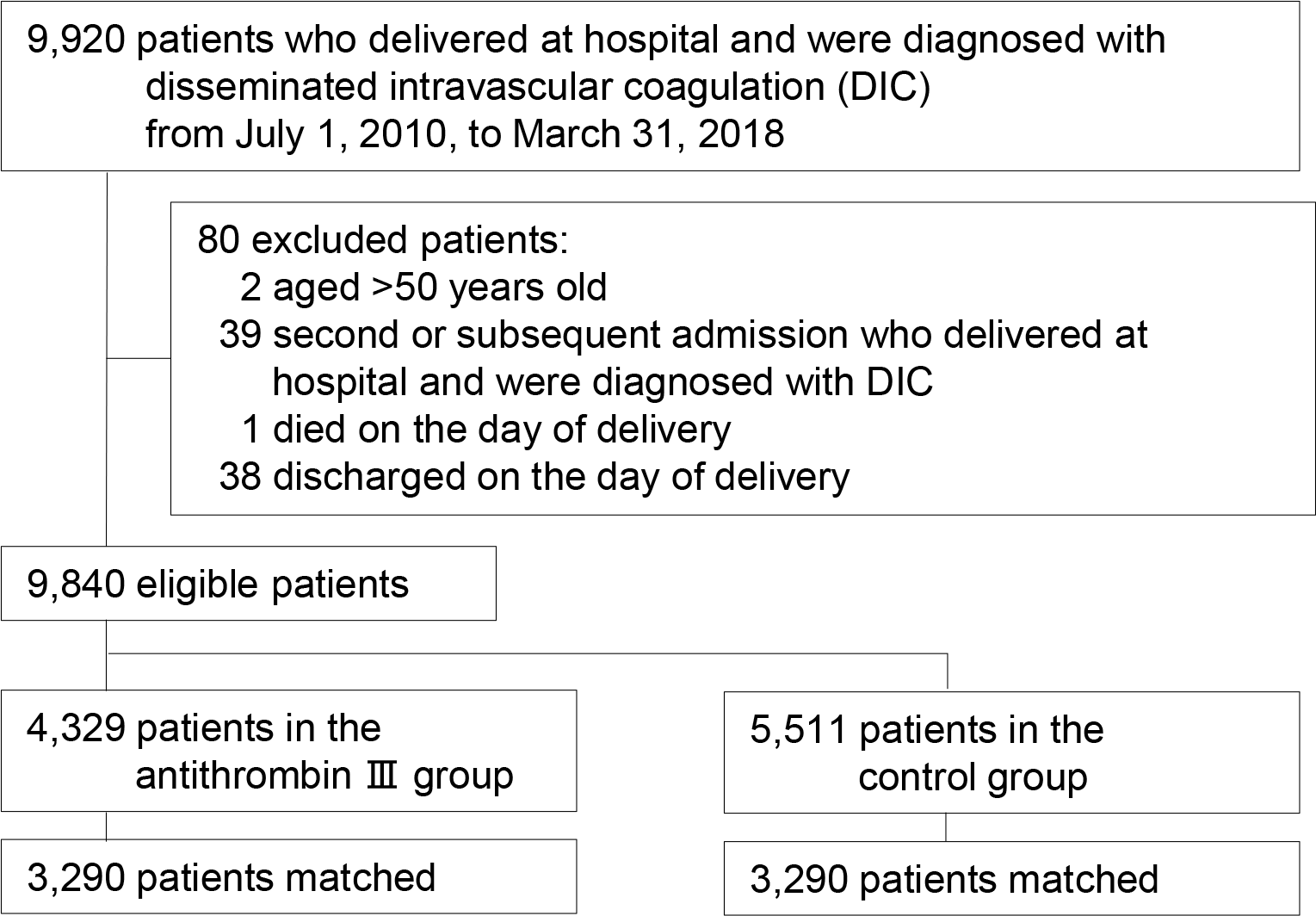
Abstract Objective: Pregnant women may develop disseminated intravascular coagulation (DIC), possibly resulting in massive maternal haemorrhage and perinatal death. The Japan guideline recommends use of antithrombin Ⅲ (ATⅢ) for DIC in obstetrics; however, its effect remains uncertain. The present study therefore aimed to investigate the effect of ATⅢ for DIC patients in obstetrics, using a national inpatient database in Japan. Design: Nationwide observational study Setting: Japan Population: We used the Diagnosis Procedure Combination inpatient database to identify patients who delivered at hospital and were diagnosed with DIC from July 2010 to March 2018. Methods: Propensity score matching analyses were performed to compare in-hospital maternal mortality and hysterectomy during hospitalization between users and non-users of ATⅢ on the day of delivery. Main Outcome Measures: In-hospital mortality, hysterectomy Results: A total of 9,920 patients were enrolled, including 4,329 patients (44%) who used ATⅢ and 5,511 patients (56%) who did not use ATⅢ. One-to-one propensity score matching created 3290 pairs. In-hospital maternal mortality did not differ significantly between the propensity-matched groups (0.3% in the ATⅢ group vs. 0.5% in the control group; odds ratio, 0.73; 95% confidence interval, 0.35–1.54). Patients in the ATⅢ group, compared with those in the control group, had a significantly lower proportion of receiving hysterectomy during hospitalization (5.3% vs. 8.7%; difference, -2.9%; 95% confidence interval, -4.2 to -1.6%). Conclusions: The present study did not show mortality-reducing effect of ATIII for patients with DIC in obstetrics. ATⅢ may have clinical benefit in terms of reduction in receiving hysterectomy.