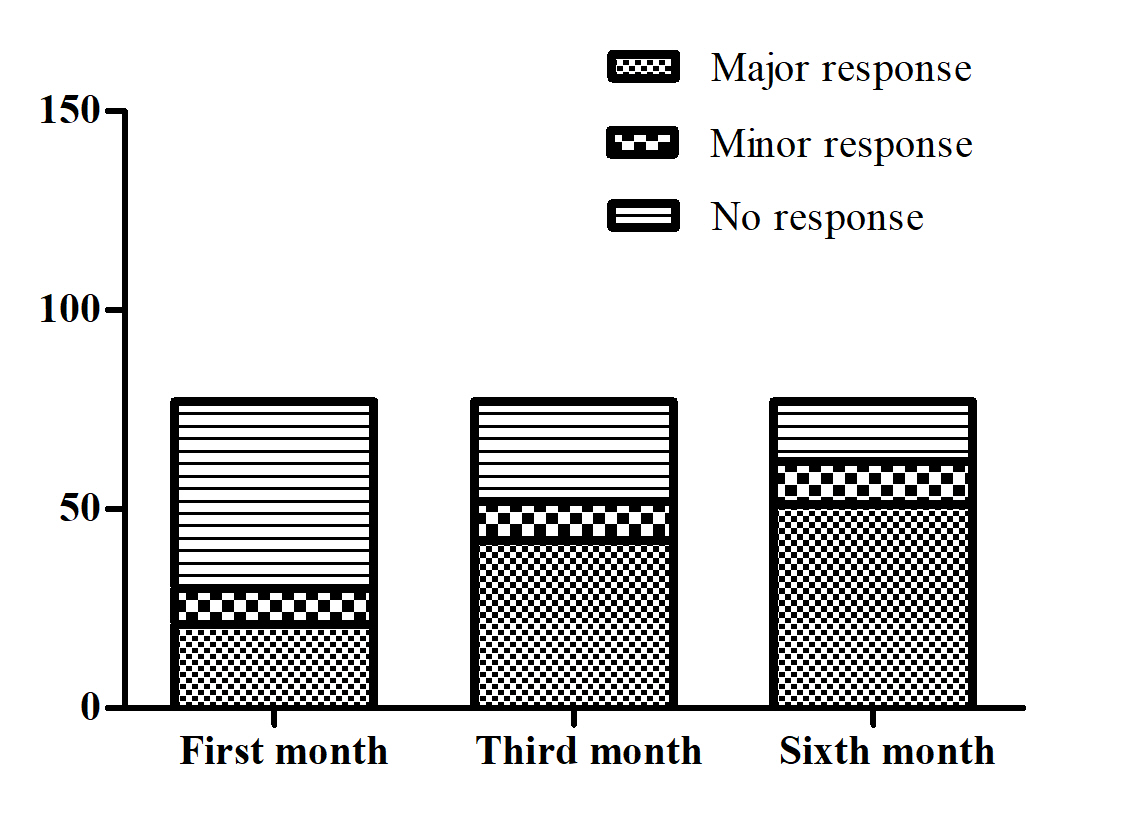
Background Thalidomide has been reported as a promising treatment for reducing transfusion volume in adults with β-thalassemia. However, the evidence about the safety and efficacy of thalidomide on children with transfusion dependent β-thalassemia (TDT) is scarce. Methods Seventy-seven children with TDT treated with thalidomide at least for 6 months were included and retrospectively analyzed. Oral dose was started at 2.5 mg•kg-1•d-1 Blood volume for maintenance of hemoglobin above 90 g•L-1 compared with pre-treatment volume is the evaluation index for response. Results After the sixth month treatment, 51/77 (66.2%) maintained Hb over 90 g•L-1 without transfusion. Adverse events were reported in 48 (63.2%) patients.Age, sex, genotype category, dosage and transfusion interval before thalidomide treatment were not correlated to treatment response. The AUC was 0.806 for the HbFat the third month of treatment in predicting probability of major responders at the sixth month treatment. Based on Youden’s index algorithm in the ROC curve, 47.298 g•L-1 was the optimal cut-off value of the HbFat the third month of treatment in predicting major responders at the sixth month treatment, with sensitivity of 67.5%, specificity of 93.3%. Conclusions The dose of thalidomide between 2.5 mg•kg-1•d-1to 3.6 mg•kg-1•d-1 is effective in TDT children. Severe side effects are uncommon. HbF concentration of 47.298 g•L-1 at the third month is recommended as the predictor for further major responders.