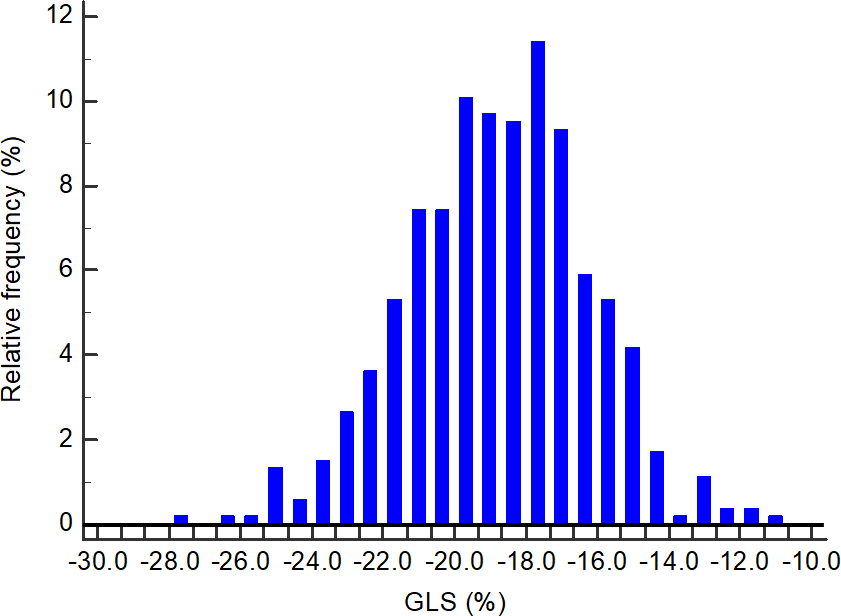
Aims: We have previously shown that 2-dimentional strain is not a useful tool for ruling out acute coronary syndrome (ACS) in the emergency department (ED). The aim of the present study was to determine whether in patients with suspected ACS, global longitudinal strain (GLS), measured in the ED using 2-dimensional strain imaging, can predict long-term outcome. Methods: Long-term (median 7.7 years [IQR 6.7-8.2]) major adverse cardiac events (MACE; cardiac death, ACS, revascularization, hospitalization for heart failure or atrial fibrillation) and all-cause mortality data was available in 525/605 patients (87%) enrolled in the Two-Dimensional Strain for Diagnosing Chest Pain in the Emergency Room (2DSPER) study. The study prospectively enrolled patients presenting to the ED with chest pain and suspected ACS but without a diagnostic ECG or elevated troponin. GLS was computed using echocardiograms performed within 24 hours of chest pain. MACE of patients with worse GLS (> median GLS) was compared to patients with better GLS ( median GLS). Results: Median GLS was -18.7%. MACE occurred in 47/261 (18%) of patients with worse GLS as compared with 45/264 (17%) with better GLS, adjusted HR 0.87 (95% CI 0.57-1.33, P=0.57). There was no significant difference in all-cause mortality or individual end-points between groups. GLS did not predict MACE even in patients with optimal 2-dimensional image quality (n=164, adjusted HR=1.51, 95% CI 0.76-3.0). Conclusions: GLS did not predict long-term outcome in patients presenting to the ED with chest pain and suspected ACS, supporting our findings in the 2DSPER study.