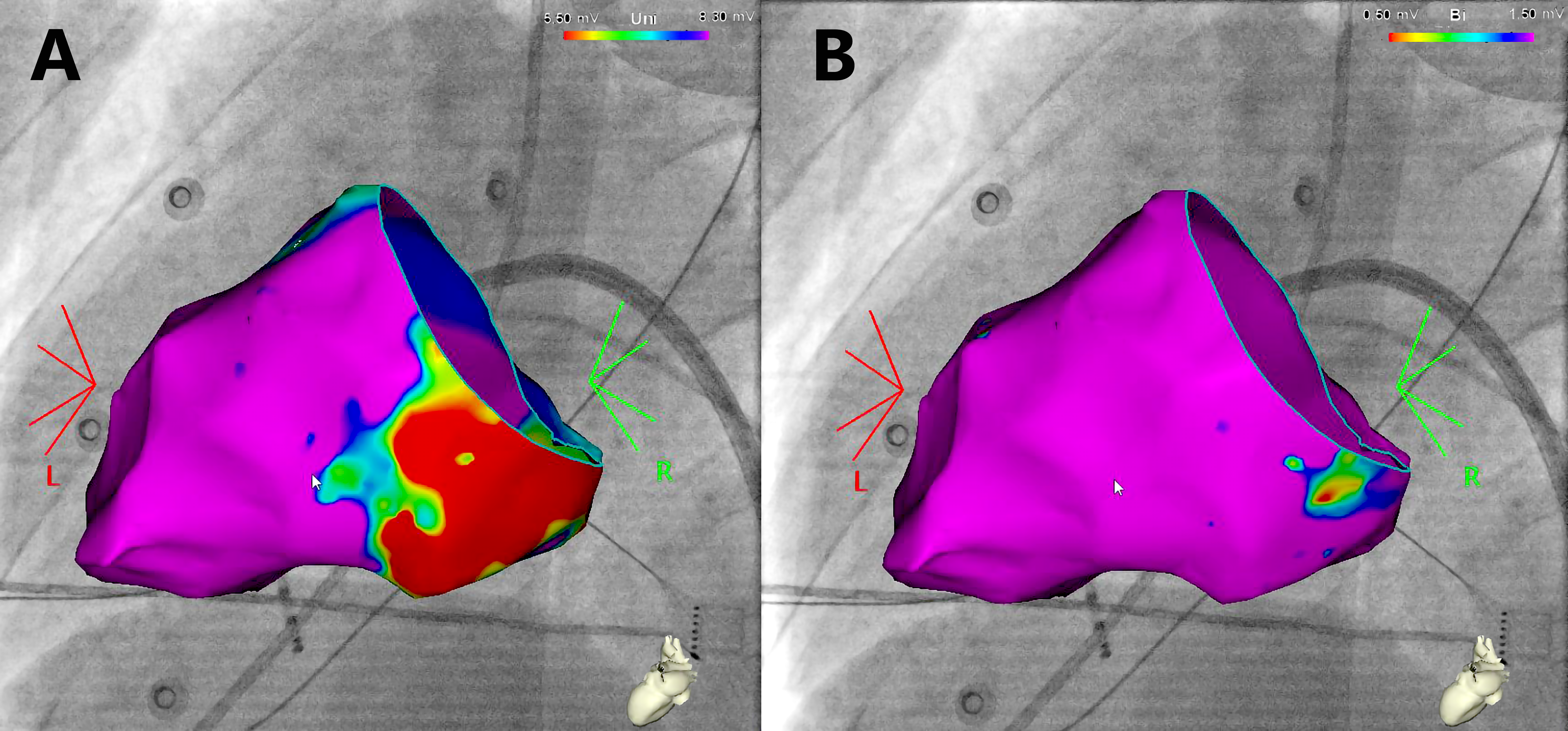
BACKGROUND. Myxomatous mitral valve prolapse (MVP) and mitral-annular disjunction (Barlow disease) are at-risk for ventricular arrhythmias (VA). Fibrosis involving the papillary muscles and/or the infero-basal left ventricular (LV) wall was reported at autopsy in sudden cardiac death (SCD) patients with MVP. METHODS AND RESULTS: Twenty-three patients with VA were enrolled, including five with syncope and four with a history of SCD. Electrophysiological parameters were correlated with VA patterns, ECG inferior negative T wave (nTW), and late gadolinium enhancement (LGE) assessed by cardiac magnetic resonance. Premature ventricular complex (PVC) burden was 12061.9±12994.6 /24 hours with a papillary-muscle type (PM-PVC) in 18 patients (68%). Twelve-lead ECG showed nTW in 12 patients (43.5%). A large Uni<8.3mV area (62.4+/- 45.5 cm2) was detected in the basal infero-lateral LV region in 12 (73%) patients, and in the papillary muscles (2.2+/-2.9 cm2) in 5 (30%) of 15 patients undergoing EAM. A concomitant Bi<1.5 mV area (5.0±1.0 cm2) was identified in 2 patients. A history of SCD, and the presence of nTW, and LGE were associated with a greater Uni<8.3mV extension: (32.8+/-3.1 cm2 vs. 9.2+/-8.7 cm2), nTW (20.1+/-11.0vs.4.1+/-3.8cm2), and LGE (19.2 ± 11.7 cm2 vs. 1.0 ± 2.0 cm2, p=0.013), respectively. All patients with PM-PVC had a Uni<8.3mV area. CONCLUSIONS: Low unipolar low voltage areas can be identified with EAM in the basal infero-lateral LV region and in the papillary muscles as a potential electrophysiological substrate for VA and SCD in patients with MVP and Barlow disease phenotype