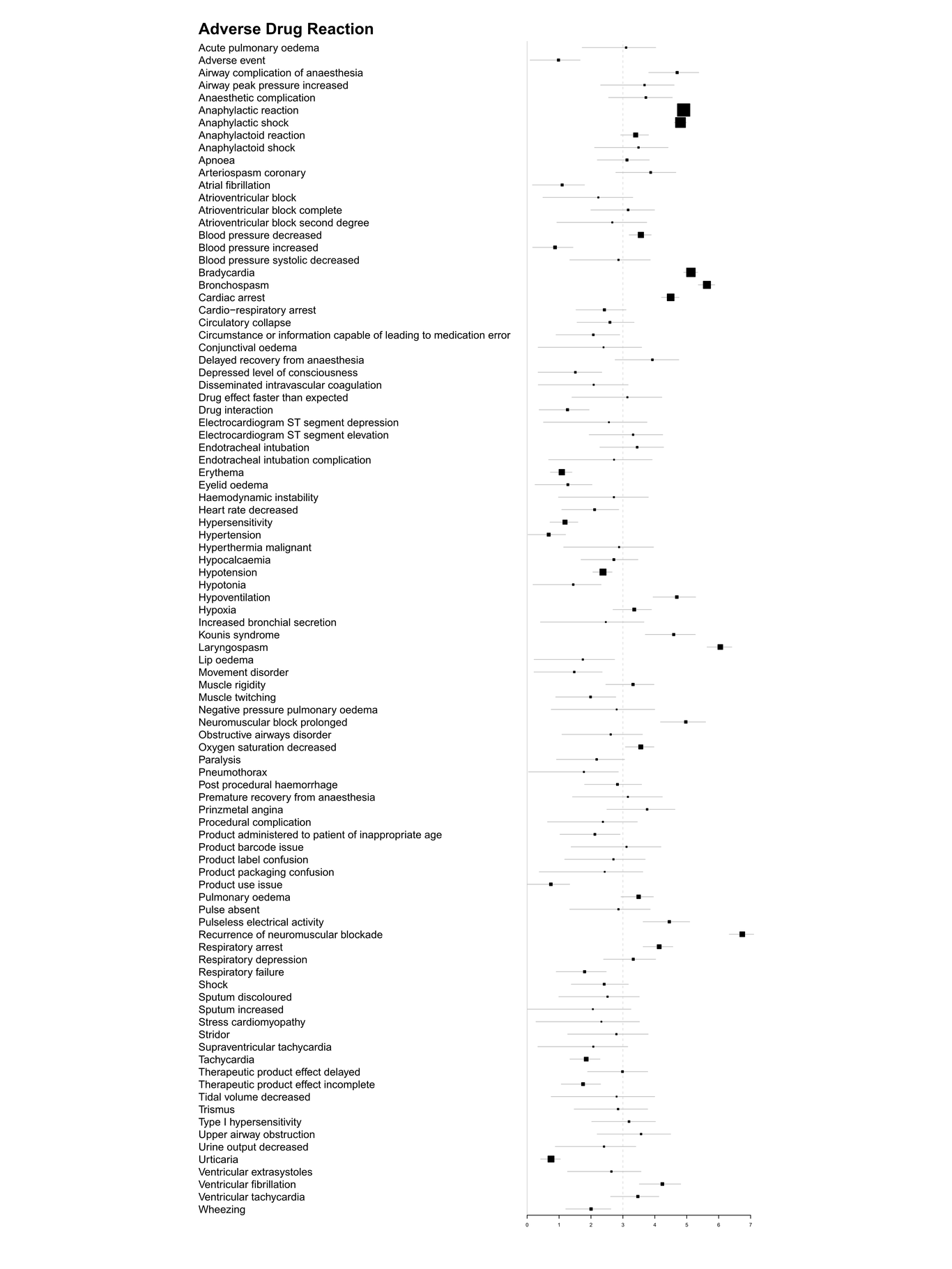
Aim: Residual neuromuscular blockade is a common complication after general anaesthesia. Sugammadex can reverse the action of aminosteroid neuromuscular blockers. Our study aimed to explore sugammadex safety issues in the real world and determine the spectrum of adverse reactions. Methods: All sugammadex-related adverse events reported in VigiBase between 2010 and 2019 were classified by group queries according to the Medical Dictionary for Regulatory Activities. A disproportionality analysis of data was performed using the information component (IC); positive IC values were deemed significant. Results: Overall, 16,219,410 adverse events were reported, and 2032 were associated with sugammadex. The most frequent reactions were recurrence of neuromuscular blockade (n = 54, IC: 6.74, 95% credibility interval [CI]: 6.33–7.10), laryngospasm (n = 53, IC: 6.05, IC025:5.64), bronchospasm (n = 119, IC: 5.63 , IC025:5.36), and bradycardia (n = 169, IC: 5.13, IC025:4.90). Fatal cases were more likely with cardiac disorders, especially in patients over 65 years. In addition, the common adverse drug reactions (ADRs) differed between different age groups (P < 0.01). The ADRs were higher between 0–17 years than in other age groups. The onset time of common ADRs was typically within one day, and 68.9% occurred within half an hour after sugammadex administration. Conclusions: Anaesthesiologists should carefully monitor the anaesthesia recovery period to correct the adverse drug reactions caused by sugammadex and recommend monitoring neuromuscular function throughout the anaesthesia process. Sugammadex should be used carefully in patients with cardiovascular diseases, and ECG and hemodynamic changes monitored after medication.