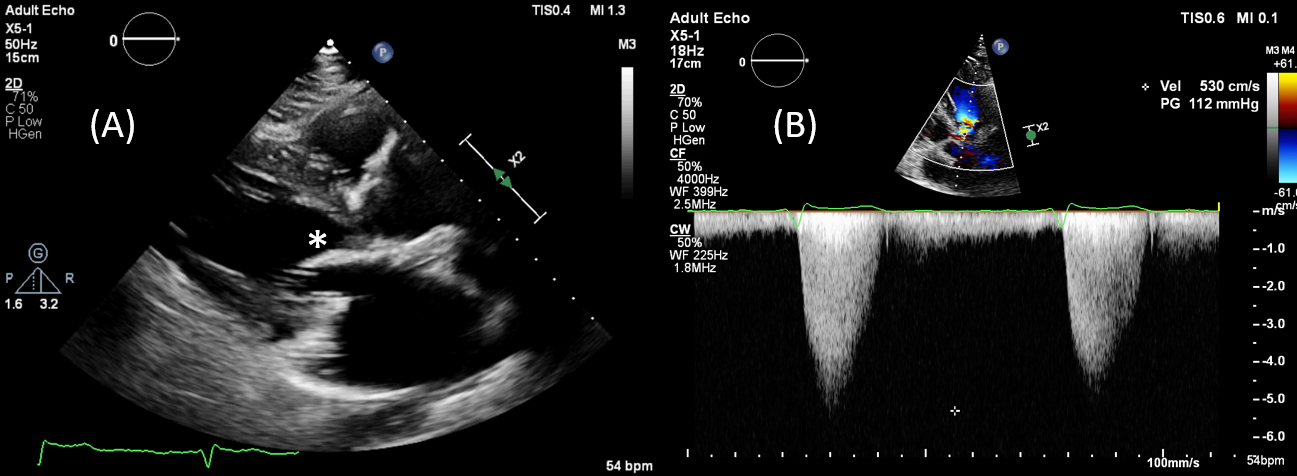
A 54-year old woman with history of hypertension was admitted our hospital with NYHA class 2-3 dyspnea. Fifteen years ago, she had primum atrial septal defect repair, septal myectomy and anterior mitral leaflet repair. Transthoracic echocardiography revealed a 112 mmHg gradient at rest in the left ventricular outflow tract (LVOT), suggesting the subaortic membrane. When transesophageal echocardiography was performed, it was observed that there was no subaortic membrane, but tunnel-type obstruction due to septal bulging in the left ventricular outflow tract. It was understood that this obstruction also contributed to the abnormally located papillary muscle, which is directly connected to the anterior mitral leaflet. The patient was evaluated as partial type Atrioventricular Septal Defect (AVSD) with a history of previous operation, anomaly of the anatomy of LVOT and atrioventricular valves, and other available findings, and the patient underwent mitral valve replacement with septal myectomy. After the operation, the lvot gradient decreased, the symptoms of the patient regressed and the patient was followed up medically.