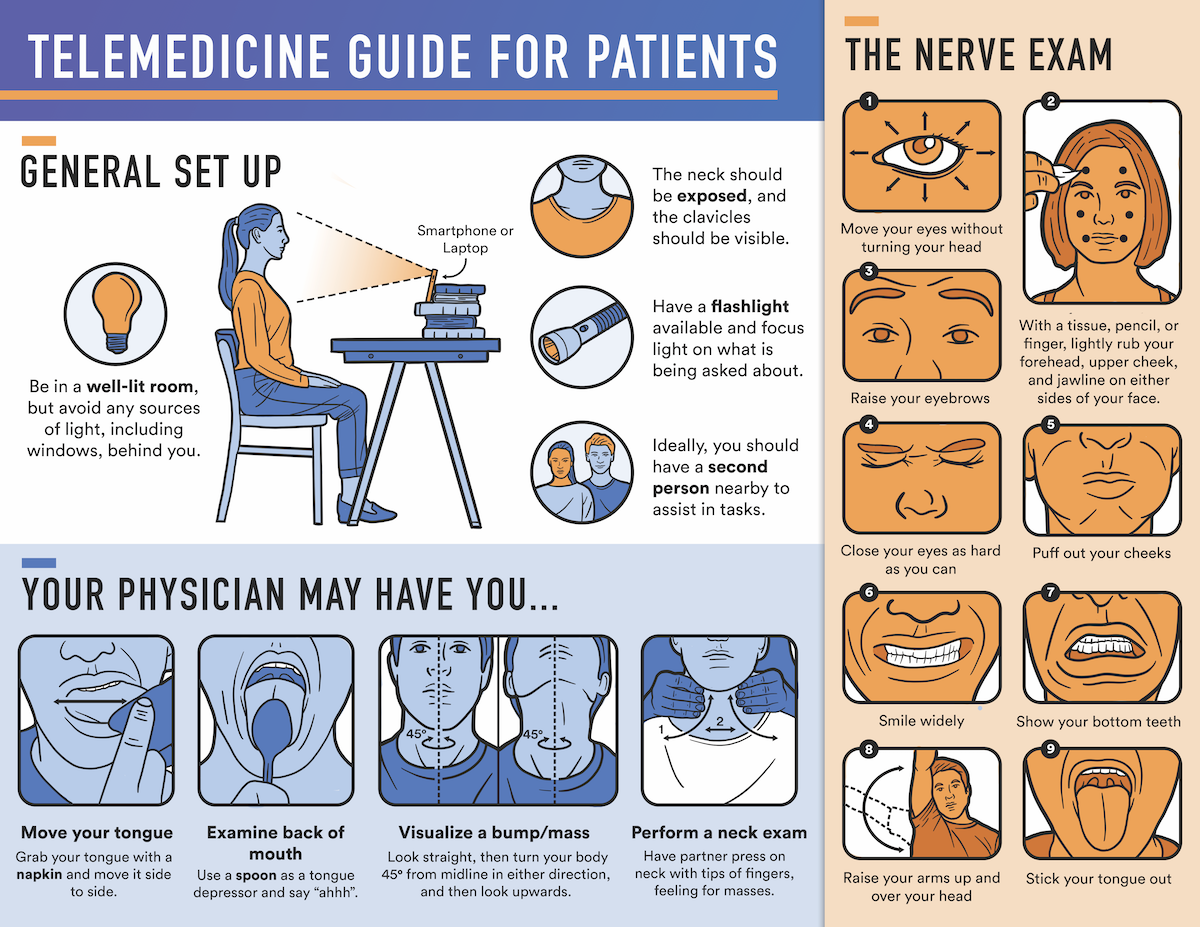
Introduction:The 2019 novel coronavirus disease (COVID-19) was initially identified in December 2019 in Wuhan, China. Following its spread across the globe within a matter of months, the World Health Organization classified COVID-19 as a pandemic.1 Its rapid transmission and high hospitalization rate have forced health professionals to drastically alter their practices in order to slow its proliferation. The rapid influx of COVID-19 related admissions in hospitals around the United States has led to a widespread shortage of crucial healthcare resources, particularly personal protective equipment (PPE), ventilators, and free ICU beds. Surgical procedures further deplete such resources in a time of acutely high need. Additionally, evidence has shown that healthcare workers may be particularly susceptible to infection from the causative pathogen, SARS-CoV-2, with roughly 20% of exposed professionals becoming infected in Italy.2Following these developments, the Centers for Disease Control and Prevention (CDC) recommended that all inpatient facilities postpone or cancel any elective surgeries.3 In the ensuing weeks, the American College of Surgeons and the American Academy of Otolaryngology-Head and Neck Surgery followed suit with this recommendation.4,5Furthermore, many hospitals and practices have opted to cancel in-person outpatient clinic visits, where patients oftentimes receive critical longitudinal care. Like other surgeons, otolaryngologists, and specifically head and neck surgical oncologists, have been deeply affected by these drastic measures. It is evident, however, that physicians must find ways to continue to monitor such patients’ conditions or treat them in some aspect. The popularity and prevalence of telemedicine has grown rapidly during this pandemic as many physicians have sought ways to maintain a continuum of care with their patients.6 Such initiatives have previously been shown to decrease costs, decrease visit time, and lead to high patient satisfaction in surgical fields.7,8Within otolaryngology specifically, certain telehealth assessments have been shown to allow for quicker examinations without compromising the communication of crucial information from the patient to the physician, or vice versa.9 However, the rapid implementation of telehealth has been a relatively new phenomenon during the COVID-19 pandemic, meaning that physicians oftentimes have to learn how to optimize their virtual visits to maximize their efficiency and effectiveness. In otolaryngology, telemedicine has not been routinely used to evaluate patients, despite estimates that 62% of otolaryngology patients would be amenable to virtual appointments.10Thus, it may be difficult for physicians to anticipate barriers to their care during a telehealth visit. Based on the authors’ experience, there exists a steep learning curve following the onset of such visits due to a variety of factors on both the patient’s and physician’s side.To our knowledge, there are no set guidelines or best practices for patients or head and neck cancer physicians conducting virtual visits. Drawing upon our experience, we aim to compile a set of guidelines for physicians and patients alike to navigate telehealth visits during the era of COVID-19. We also created a handout that can be distributed to patients prior to the visit, such that patients can familiarize themselves with general expectations and key examination steps that they may be asked to perform during the visit.