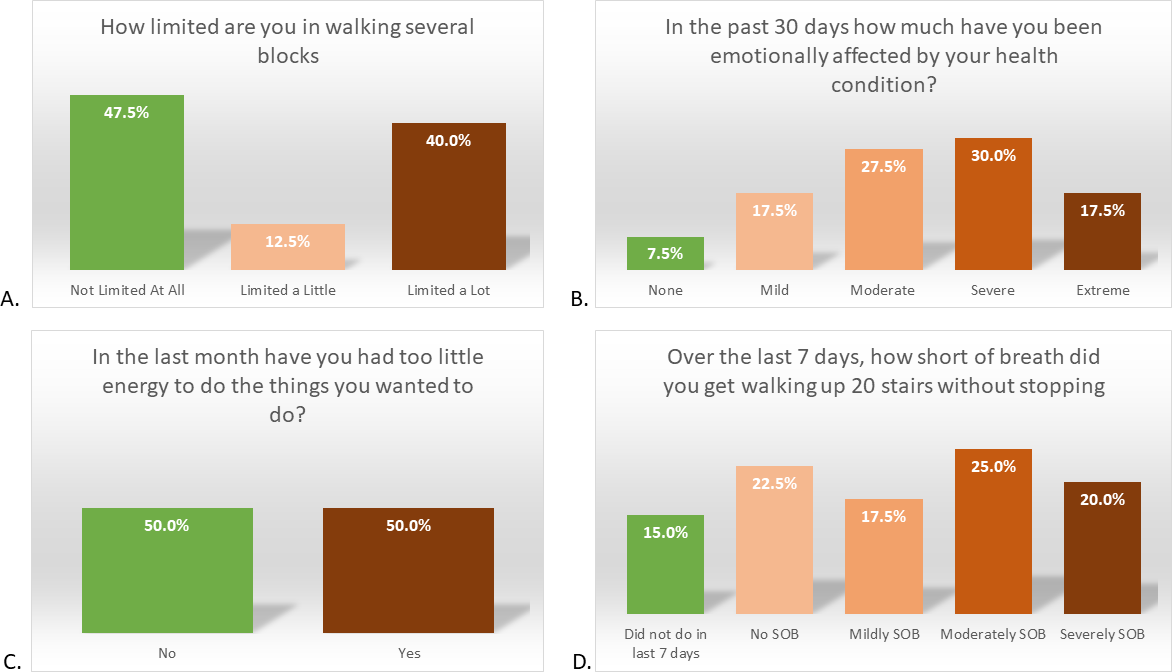
Over 645 million people worldwide have been infected with SARS-CoV-2, the virus that causes COVID-19. Critical knowledge gaps regarding the characteristics, duration, and impact of symptoms due to “long COVID”. This study evaluated the persistence of symptoms at one year following hospitalization with COVID-19, comparing responses on standardized measurement tools to population norms. Adults hospitalized with COVID-19 March-October 2020 during the initial emergence period in Southeast Michigan were eligible. A detailed survey was conducted via telephone 9-15 months after hospital discharge. Questions assessed fatigue, dyspnea, and physical functioning related to their COVID-19 illness. The median World Health Organization Disability Assessment Schedule (WHODAS) polytomous score placed 50% (n=20/40) of participants in the 90 th percentile of disability based on population norms. The mean SF-36 physical functioning score was almost nine points below population norms (mean=70.6, standard deviation=27.4). Additionally, 47.5% of individuals (n=19) were severely emotionally affected by their health condition. Over half of participants surveyed were still impacted a year after initial infection, experiencing limited functional ability, fatigue, and emotional difficulties. Given the impact of these symptoms on day-to-day quality of life, further studies are needed to develop strategies for treatment and management of post-COVID conditions.