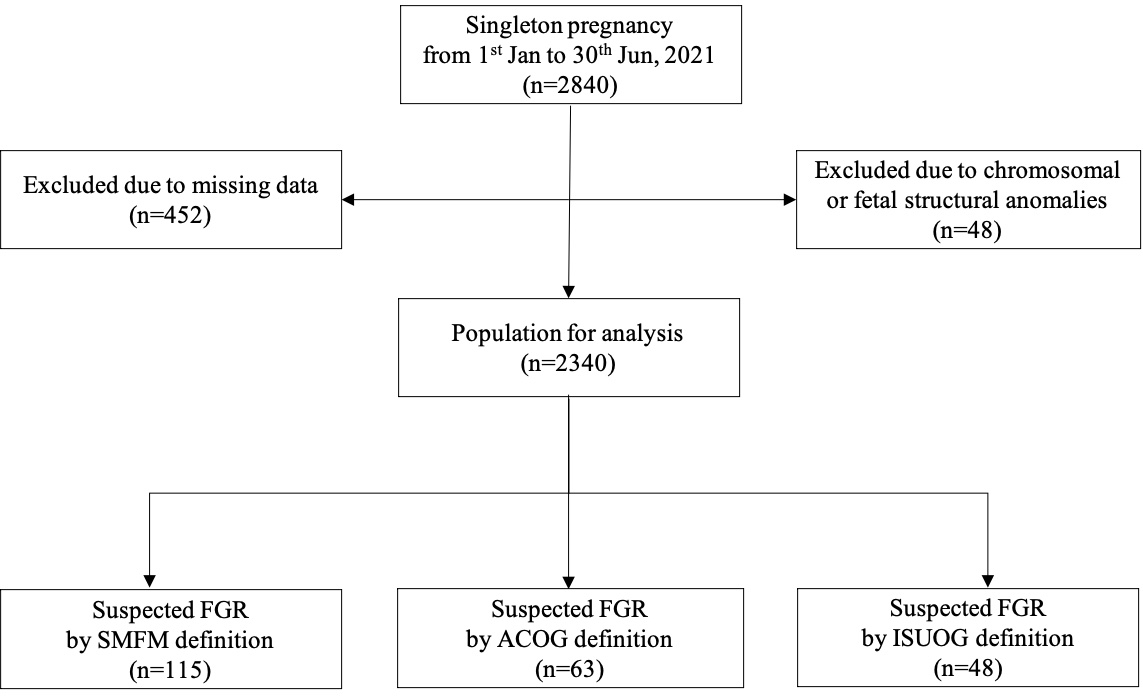
Background Fetal growth restriction (FGR) is defined differently by the American College of Obstetrics and Gynecology (ACOG), Society for Maternal-Fetal Medicine (SMFM), and the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG). Objective The purpose of this study was to investigate the predictive effect of three different diagnostic criteria of FGR on small-for-gestational-age (SGA) and adverse neonatal outcome (ANO), so as to find a better FGR-definition for Chinese population. Study Design The clinical data of singleton pregnancy who received regular pregnancy care and gave birth at the Department of Obstetrics and Gynecology of Peking University First Hospital from January 1, 2021, to June 30, 2021 were collected. FGR cases were determined according to three different diagnostic criteria by ACOG, SMFM, or ISUOG. The primary outcome was the prediction of SGA and a composite ANO. SGA was defined as neonatal birth weight less than 10 th percentile. An ANO included one of these adverse outcomes: neonatal umbilical arterial blood pH < 7.1, 5-minute Apgar score<7, acute respiratory distress syndrome (ARDS), intraventricular hemorrhage, and neonatal convulsion, and transfer to the neonatal intensive care unit (NICU). The specificity, sensitivity, negative predictive value (NPV) and positive predictive value (PPV) of the different diagnostic criteria for SGA and ANO were compared. The discriminatory capacities of the three FGR-definitions were compared using the area under receiver-operating-characteristics curves (AUC). Results A total of 2340 cases were included in this study, and 115 (4.9%), 63 (2.7%), and 48 (2.1%) cases of FGR were diagnosed using the diagnostic criteria issued by the SMFM, ACOG, and ISUOG respectively. There were 147 (6.28%) cases of SGA neonates. The SMFM criteria had higher sensitivity (40.82% vs 24.49%, 20.41%) for SGA compared to the ACOG and ISUOG criteria. On the contrary, the ISUOG criteria had a higher specificity (99.18% vs 97.49%, 98.77%) than the SMFM and ACOG criteria for predicting SGA. A total of 127 (5.43%) cases were complicated with ANO. All three definitions had low sensitivity for ANO (17.32%, 12.6%, 11.81%) and high specificity of 95.8%, 97.88% and 98.51%. The AUCs of SMFM for predicting SGA (0.692) and ANO (0.566) were slightly higher than those of ACOG (0.616, 0.552) and ISUOG (0.598, 0.552). Conclusion The predictive value of the SMFM and ISUOG definition for SGA and ANO was better than that of the ACOG criteria. In Chinese population, the discriminatory capacities of SMFM FGR definition were superior compared to the other two definitions.