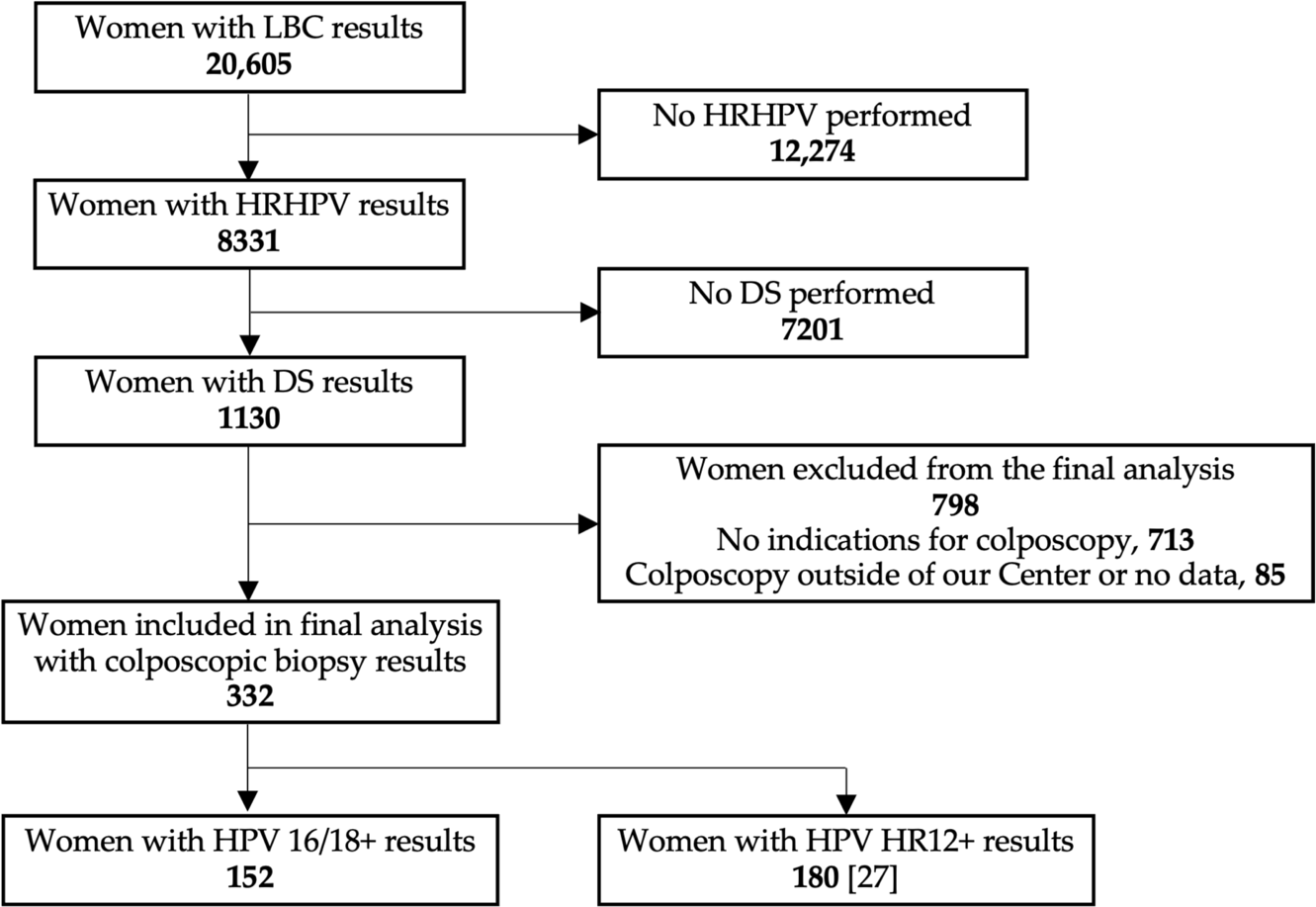
Background: Major screening abnormalities in pre-colposcopic stage are tests results that imply direct referral to colposcopy (and/or expedited treatment) without performing additional high-grade squamous intraepithelial lesions or worse (HSIL+) risk selection testing. Currently, both clinically validated HSIL+ risk selection tests, reflex cytology and reflex p16/Ki67 dual staining (DS), are being compared for use in primary HPV-based screening to avoid possible overtreatment, but there is still no sufficient data available for their performance. Methods: Among 30,066 liquid-based cervical cancer screening tests results, a group of 332 women was selected with available HRHPV tests results with 16/18 limited genotyping, liquid-based cytology, DS, and histology results from standardized colposcopy with biopsy. In HPV 16/18+ cases, three triage approaches were retrospectively analyzed. Predictive values for detection of HSIL+ were calculated and number of colposcopies required in each strategy. Results: Both triage models with DS used (reflex cytology followed by DS, and reflex DS alone in all cases) had significantly higher PPV for HSIL+ than strategy with reflex cytology alone (44.2%/45.7% vs. 28.3%; p<0.0001). In models with DS, less colposcopies were required (95/92 vs. 152) and less colposcopies were needed per HSIL+ detection (2,26/2,19 vs. 3,54). Only 1 HSIL+ case was missed in both triage models with DS incorporation. Conclusions: p16/Ki67 dual-stain may be an effective, alone or combined with cytology, triage test to detect HSIL+ in patients with major screening abnormalities in primary HPV-based cervical cancer screening. Performing cytology as the first triage test improves the strategy by enabling referrals to expedited treatment in selected cases.