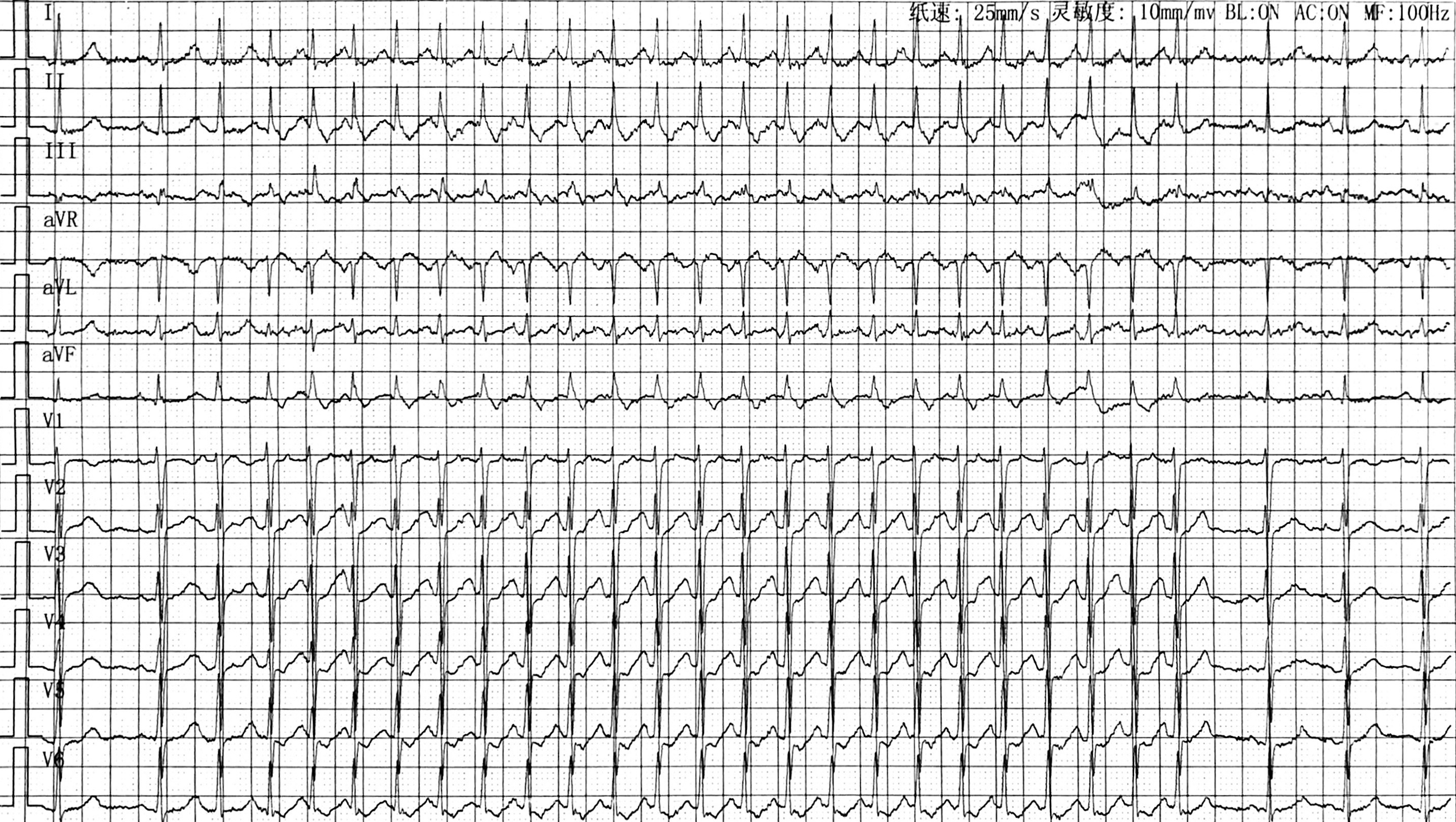
Responses to Ventricular Overdrive Pacing during Wide QRS Tachycardia: What is the Mechanism?Wentao Gu MD1, Xinping Luo MD1, Jian Li MD1, Jinjin Zhang MD1, Nanqing Xiong MD1*1. Department of Cardiology, Huashan Hospital Fudan University, 12 Wulumuqizhong Road, Jing’an District, Shanghai 200040, China*Corresponding author: Nanqing Xiong MD, Department of Cardiology, Huashan Hospital Fudan University, 12 Wulumuqizhong Road, Jing’an District, Shanghai 200040, China. E-mail: [email protected] words: wide QRS complex tachycardia, ventricular overdrive pacing, supraventricular tachycardia, AV reentrant tachycardia, orthodromic His activationFunding: (None)A 35-year-old female presenting with recurrent palpitation was referred for electrophysiology study. Short episodes of narrow QRS tachycardia could be recorded on ECG (Figure 1). During electrophysiology study, the tachycardia could be readily induced with atrial pacing or programmed atrial extrastimuli, but usually terminated in seconds, making it difficult to perform diagnostic maneuvers. When it spontaneously changed to a wide QRS tachycardia, a burst of ventricular overdrive pacing (VOD) was delivered which turned it back to the narrow complex one (Figure 2). What can be learned from the response?The first 4 beats in this tracing showed wide complex tachycardia (WCT) with right bundle branch block (RBBB) morphology and 1:1 ventriculo-atrial ratio. Candidates for diagnosis could be ventricular tachycardia, supraventricular tachycardia (SVT) with RBBB, bundle branch reentrant tachycardia and preexcited tachycardia. An H-V interval of 53ms approximating that during sinus rhythm excluded ventricular tachycardia from myocardium and preexcited tachycardia. The last 4 beats were clinical narrow complex tachycardia with the same cycle length, H-V interval and atrial activation sequence (earliest A at CS7-8) as the WCT, highly indicating that the WCT was SVT with functional RBBB caused by continuous concealed activation from left bundle branch before VOD peeled back the refractoriness of the right bundle branch in the following beats. In addition, A right-sided accessory pathway (AP) was unlikely given the same H-A interval (127ms, measured to CS7-8) with and without RBBB [1].The middle 4 beats demonstrated progressive change in QRS, from fusion to probable fully-paced morphology during VOD. The 3rdbeat advanced the subsequent A without atrial activation change, indicating the presence of a septal AP. However, post-pacing interval (PPI) was 125ms over tachycardia cycle length (TCL) with V-A-H-V response, which argued against AV reentrant tachycardia (AVRT) utilizing a septal AP. Note that His signal was found after the 3rd and the 4th stimulating artifact. Considering the extremely short interval between the 3rd artifact and the subsequent His (17ms), it could hardly be a retrograde His, but was activated in an orthodromic direction instead. A progressively increased A-H interval after the 2nd, 3rd and 4thpacing suggested decremental conduction in AV node before orthodromic His capture. When atrium was entrained, anterograde conduction to the His bundle during VOD supported the diagnosis of AVRT and excluded AV nodal reentry [2]. The long PPI was associated with the delay of the first return His-V following VOD-induced decremental AV nodal conduction. The corrected PPI-TCL was 78ms after subtracting the difference between the first return A-H and tachycardia A-H from PPI [3]. The AP was successfully ablated at left posterior septum, which rendered the tachycardia non-inducible.