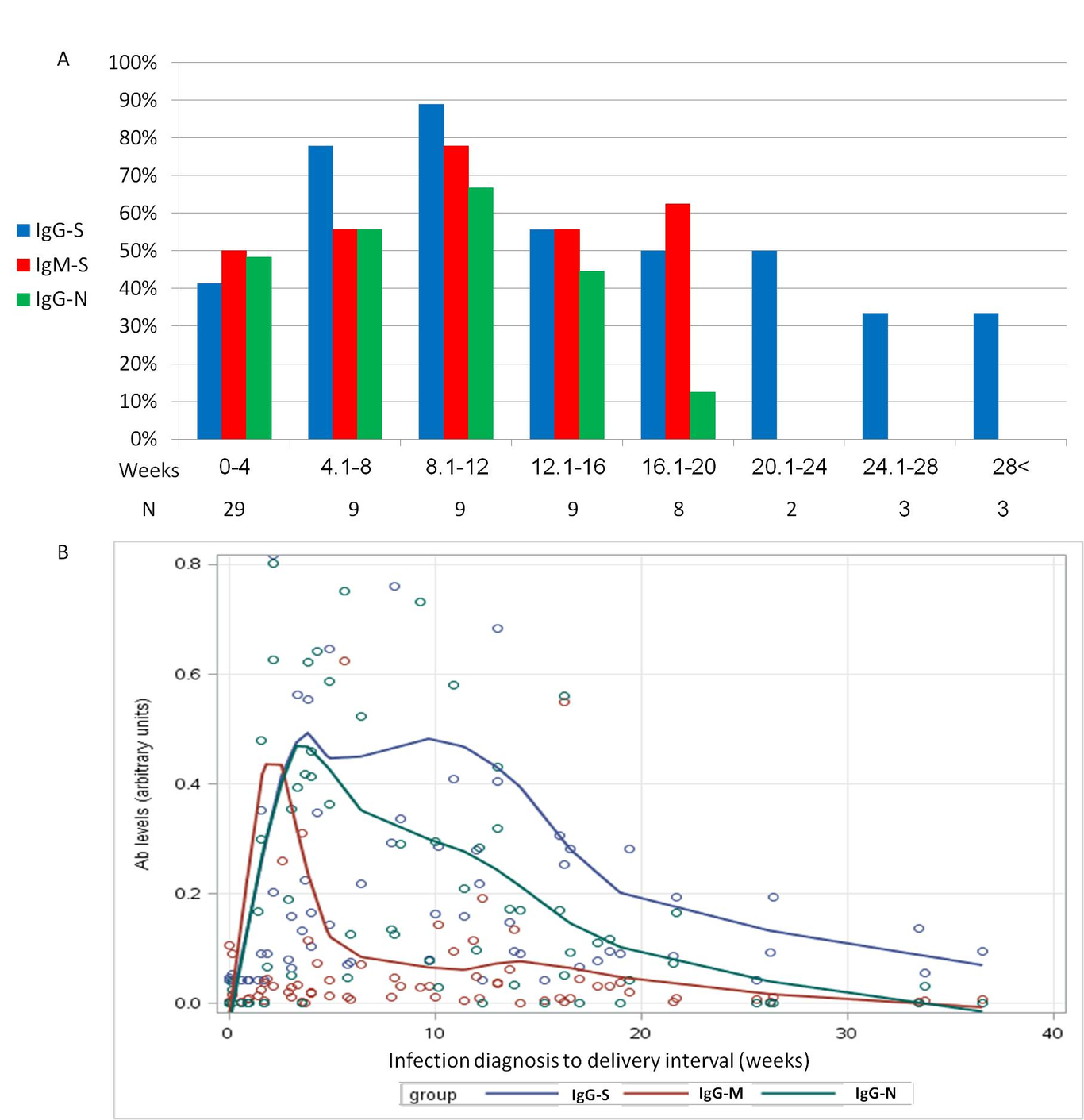
Objective: To explore maternal humoral immune responses to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and the rate of vertical transmission. Design: A prospective cohort study. Setting: Two university-affiliated medical centers in Israel. Population: Women positive for SARS-CoV-2 reverse-transcription-polymerase-chain-reaction (RT-PCR) test, during pregnancy were enrolled just prior to delivery. Methods: Levels of anti-SARS-CoV-2 spike-IgM, spike-IgG and nucleocapsid-IgG were tested in maternal and cord blood at delivery, and neonatal nasopharyngeal swabs were subjected to PCR testing. Main outcomes measures: The primary endpoint was the rate of vertical transmission, defined as either positive neonatal IgM, positive neonatal IgG with sero-negative mother or positive neonatal PCR. Results: Among 72 women, 36 (50%), 39 (54%) and 30 (42%) were positive for anti-spike-IgM, anti-spike-IgG and anti-nucleocapsid-IgG, respectively (p<0.0001 for IgG antibodies-comparison). At least 8/72 (11%) neonates were infected in utero; one had a positive PCR result and seven had positive IgG antibodies while their mothers were seronegative for the same IgG. IgM was not detected in cord blood. Anti-nucleocapsid-IgG and anti-spike-IgG were detected in 83% and 85% of neonates of seropositive mothers, respectively (Pearson coefficient correlation 0.8, p<0.001). The highest rate of positive maternal serology tests was 8-12 weeks post-infection (89% anti-spike IgG, 78% anti-spike-IgM and 67% anti-nucleocapsid-IgG). Thereafter, the rate of positive serology tests declined gradually; at 20 weeks post-infection, only anti-spike-IgG was detected in 33-50%. Conclusions: The rate of vertical transmission was at least 11%. Vaccination should be considered 3 months post-infection in pregnant women due to a decline in antibody levels.