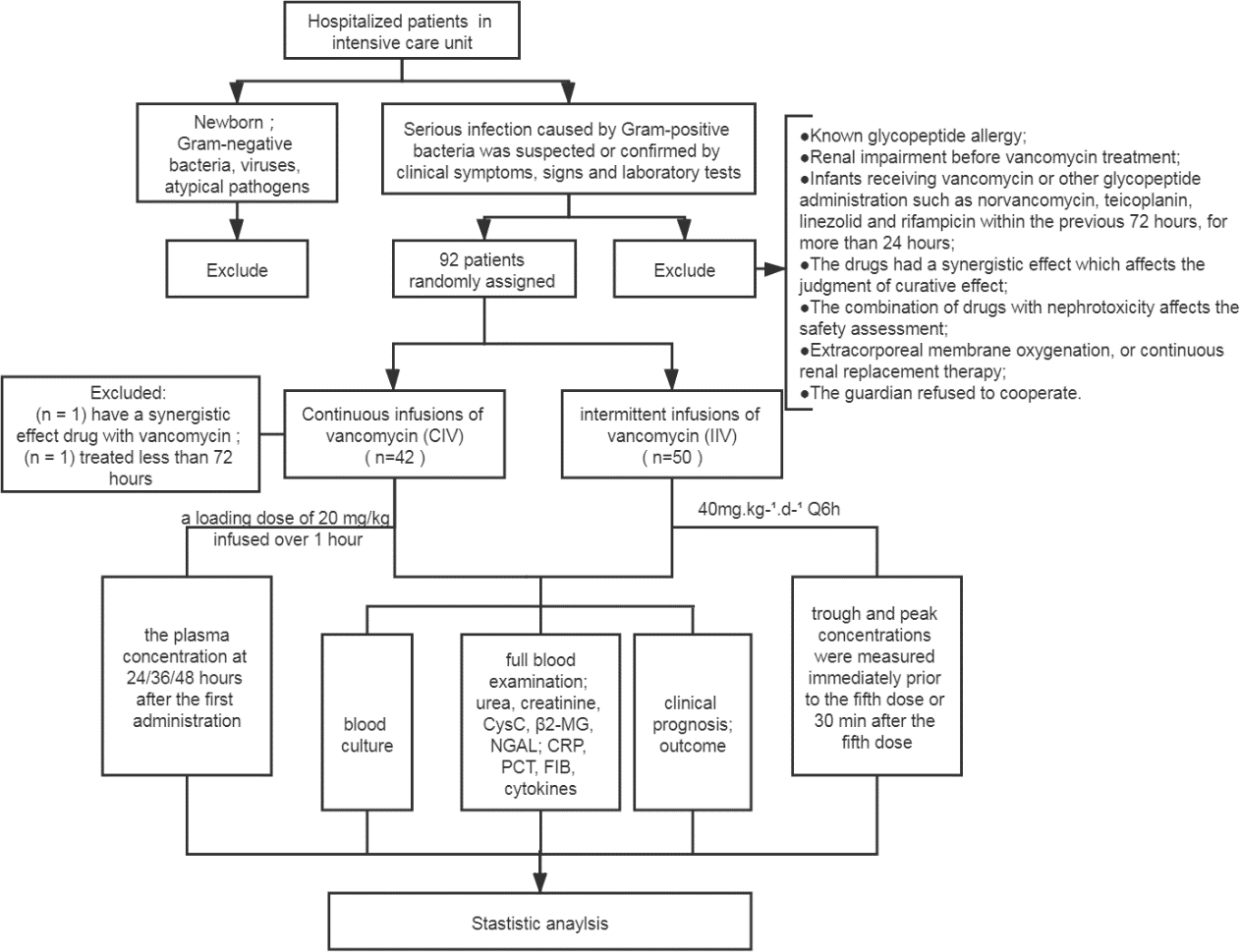
Objectives This study aimed: (a) to compare the effects of continuous and intermittent infusions of vancomycinon the pharmacodynamics/pharmacokinetics (PK/PD) at a dose of 40 mg.kg-1.d-1 in children; (b) to compare the outcomes and the frequency of the drug-related adverse effects in this population. Methods This single-center randomized controlled trial enrolled children, admitted to the intensive care unit over a period of 36 months (June 1, 2017–June 1, 2020), and required vancomycin therapy. These children were randomly assigned to the CIV and IIV groups. The demographic, indices of PK/PD, outcomes, and drug-related adverse effects were collected and analyzed. Results Of the 92 patients randomized, 90 were included in the analysis and 2 patients dropped out of the trial. The study was conducted on two groups: the IIV group (n = 50) and the CIV group (n = 40) and various parameters were compared. The plateau concentration in the CIV group was higher than the trough concentration in the IIV group (15.22 mg.L-1 vs. 6.25 mg.L-1, P < 0.05). The AUC0–24/MIC of the IIV group was lower (median 391.45, IQR 251.45–898.16) compared to that of the CIV group (429.60, IQR 220.92–769.20; P > 0.05). None of the two groups showed any significant difference in the clinical prognosis or the drug-induced nephrotoxicity. Conclusions Therefore, CIV can assist in attaining the target concentrations of vancomycin more quickly in critically ill children, without increasing the dosage. Also, the children subjected to CIV demonstrated no difference in clinical efficacy and the rate of drug-related nephrotoxicity.