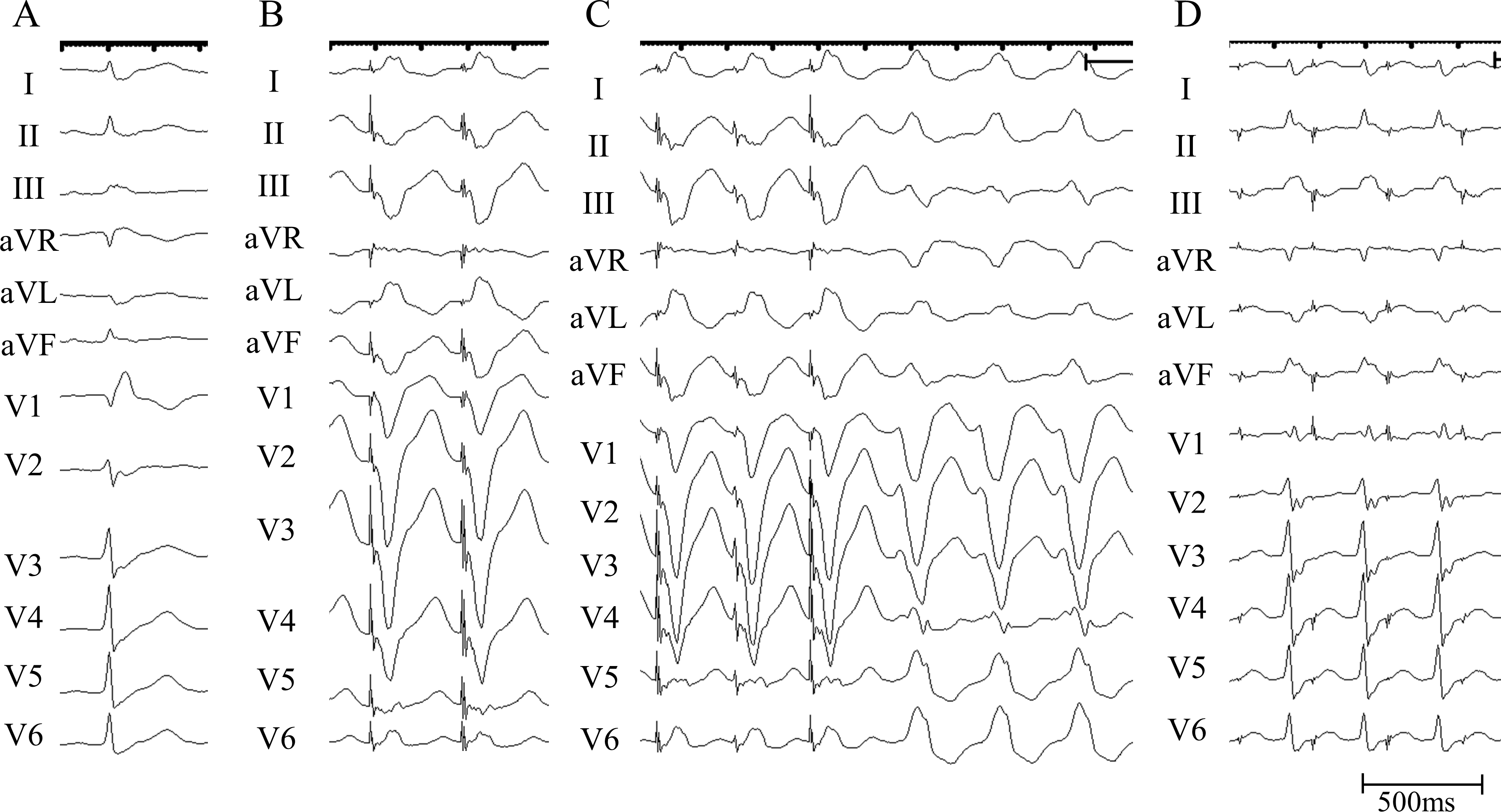
A 70-year-old man presented with regular wide QRS complex tachycardia (WCT) at a rate of 185 beats/min, characterized by left bundle branch block morphology. WCT termination was achieved through electrical cardioversion. A subsequent 12-lead electrocardiogram revealed sinus rhythm with complete right bundle branch block (CRBBB) morphology. Echocardiography showed normal left ventricular function without structural heart disease. An electrophysiological study was then conducted, followed by catheter ablation. At baseline, the atrio-His and His-ventricular intervals were normal. Fractionated ventricular potentials were observed in the para-Hisian region during sinus rhythm. Neither dual atrioventricular (AV) nodal physiology nor ventriculoatrial conduction was observed during programmed pacing. Clinical WCT was induced by ventricular extra-stimulation with concurrent AV dissociation and no visual His bundle potential, confirming the diagnosis of ventricular tachycardia (VT). Figure 1 illustrates 12-lead electrocardiograms recorded during overdrive pacing from the right ventricular apex (RVA) and right atrial septum during VT. The electroanatomical activation map revealed a distinctive focal breakout pattern with fractionated potentials originating from the para-Hisian region. In the noncoronary cusp (NCC), corresponding to the opposite side of the para-Hisian region, prolonged and fractionated ventricular potentials preceding QRS onset by 56 ms were recorded (Figure 2A). Figure 2B shows the intracardiac electrogram recorded during ventricular overdrive pacing from the NCC during VT. Based on these observations, what is the mechanisms underlying the tachycardia?