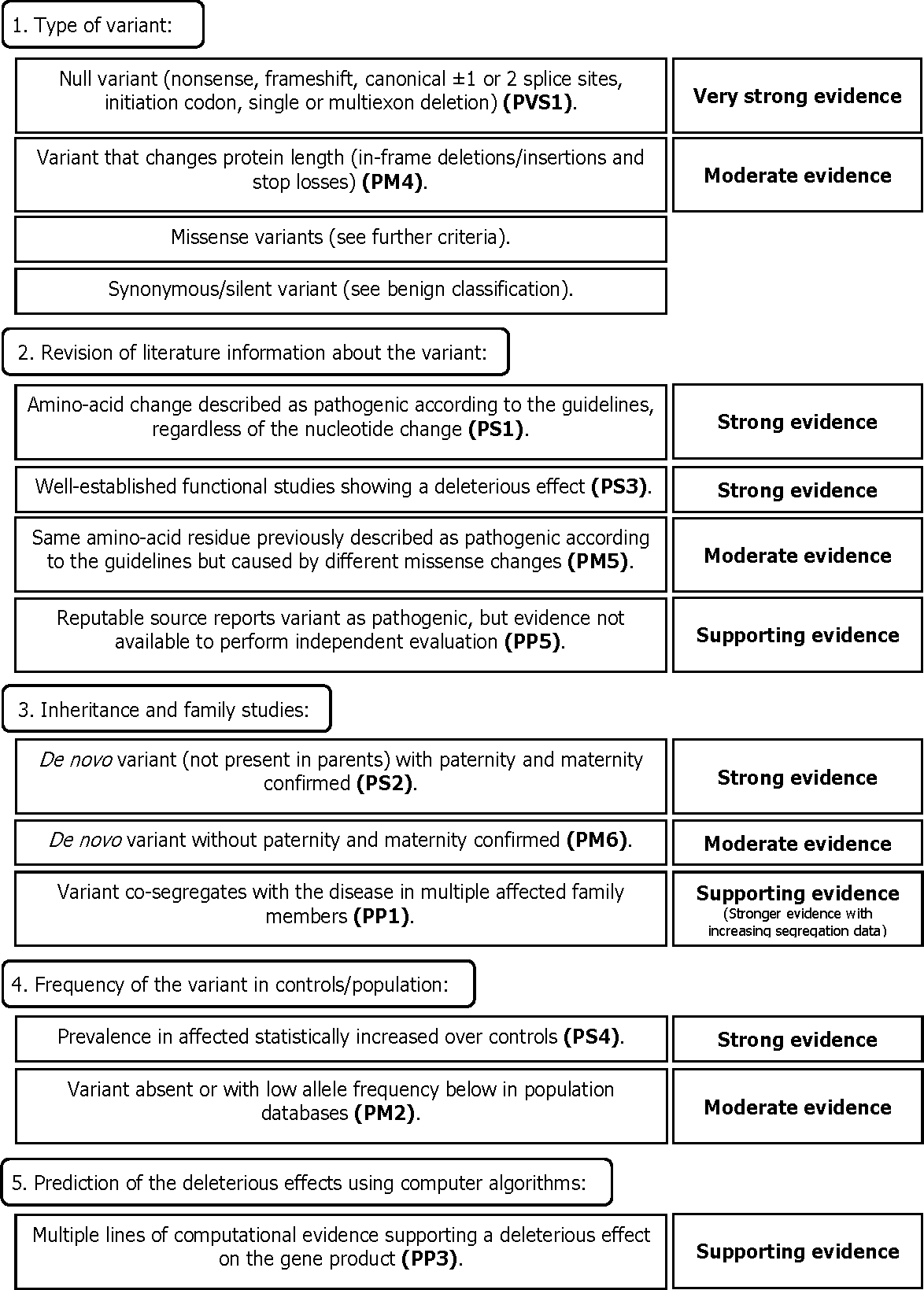
The most common form of genetic generalized epilepsy (GGE) is juvenile myoclonic epilepsy (JME), which accounts for 5 to 10% of all epilepsy cases. The gene EFHC1 is associated with JME. However, it remains debatable whether testing for EFHC1 mutations should be included in the diagnostic epilepsy gene panels. To investigate the clinical utility of EFHC1 testing, we studied 125 individuals: 100 with JME and 25 with other GGEs. We amplified and sequenced all EFHC1 coding exons. Then, we applied a revised version of the American College of Medical Genetics and Genomics (ACMG)/Association for Molecular Pathology(AMP) guidelines to predict the pathogenicity and benign impact of the variants. Mutation screening revealed 11 missense variants in 44 probands with JME (44%) and in 1 of the 7 individuals with generalized tonic clinic seizures on awakening (14%). Overall, only the variant c.685T>C was strictly classified as ‘pathogenic’ (1/11, 9%), five variants were classified as ‘benign’ (45%), and the remaining five (45%) were considered variants of uncertain significance (VUS). There is currently a limitation to test for genes that predispose an individual to complex, non-monogenic phenotypes. Thus, we consider EFHC1 to be a risk factor for JME but not currently useful for clinical purposes.