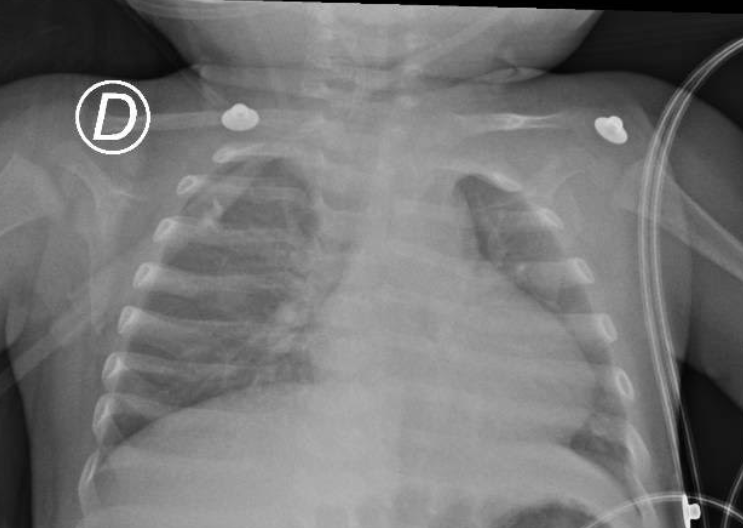
The current pandemic of the novel coronavirus SARS-CoV-2 infection has affected over 6 million humans around the planet. The clinical manifestations of Coronavirus disease 2019 (COVID-19) are diverse, ranging from asymptomatic or mild flu-like symptoms to atypical pneumonia, severe respiratory distress syndrome, systemic inflammation, immune dysregulation and dyscoagulation.Inborn errors of immunity (IEI) are a heterogenous group of more than 430 rare congenital disorders with increased susceptibility to infection, autoimmunity, atopy, hyperinflammation and cancer. Autosomal recessive ARPC1B deficiency is an actinopathy, as are DOCK8 deficiency and the Wiskott-Aldrich Syndrome. Defective actin polymerization affects hematopoietic cells, impairing their migration and immunological synapse1, which results in a combined immune deficiency characterized by leukocytosis, eosinophilia, platelet abnormalities and hypergammaglobulinemia; and clinically, by eczema and food allergy, infections caused by bacteria, fungi and viruses, vasculitis, and bleeding diathesis2.Here, we describe a male infant patient with known ARPC1B deficiency who was hospitalized for COVID-19 pneumonia and improved without requiring intensive care or mechanical ventilation.An 8-month-old infant was brought to the emergency department with high-grade fever. His family history is remarkable for one brother who died as a newborn from intracranial bleeding, and an 11-year-old sister with the same genetic defect who underwent hematopoietic stem-cell transplantation twice without success, and is currently on antimycobacterial treatment, antimicrobial prophylaxis and regular subcutaneous immunoglobulin. The patient was first seen at age 1-month old for eczema and rectal bleeding attributed to cow milk protein allergy. At age 4 months, he developed bronchiolitis caused by respiratory syncytial virus (RSV) and oral candidiasis. Laboratory workup revealed leukocytosis (17,500-33,600/mm3), eosinophilia (5,600-20,100/mm3) and a marginally high (467,000) platelet count; as well as high serum IgG (737 mg/dL) and IgA (165 mg/dL) with normal IgM (37.7 mg/dL). CD8+ T lymphocytes were low at 3% (257 cells) and B cells were elevated at 48% (4,116 cells). Whole exome sequencing identified a homozygous 46 base-pair deletion in exon 8 of ARPC1B(chr7:99,392,784 hg38; p.Glu300fs).Upon his arrival to the emergency department he was febrile with tachycardia and signs of septic shock requiring rapid fluid resuscitation. He showed no respiratory or gastrointestinal signs. He also had a post-traumatic ulcerated lesion under the tongue with dark discoloration, which raised a concern for fungal infection. Intravenous antibiotics (ciprofloxacin) with antifungal coverage were started within the first hour, and a dose of intravenous immunoglobulin (IVIG) at 1g/kg. Blood counts revealed leukocytosis, neutrophilia, and mild eosinophilia without lymphopenia, while platelets were initially found within normal limits. A day later, blood culture had grownPseudomonas aeruginosa .During his second day of hospitalization, the patient persisted febrile, tachycardic and tachypneic, with oxygen desaturation into the low 80s. Chest X-ray showed nonspecific bilateral interstitial opacities in the perihilar regions (Figure 1 ). Real-time Polymerase chain reaction (RT-PCR) for SARS-Cov2 came back positive, and he was then transferred to a COVID-19 isolation area. The potassium hydroxide (KOH) test for oral thrush was negative for yeast cells, after which amphotericin was switched to fluconazole. Supplemental oxygen was discontinued on day 6 of hospitalization, when mild thrombocytopenia and a prolonged thromboplastin time (aPTT) (but normal fibrinogen and ferritin serum levels) were reported. After completing 14 days of antimicrobial treatment, the patient was discharged without ever requiring intensive care unit admission or mechanical ventilation.The behavior of COVID-19 in patients with IEI might help dissect the immune response to SARS-Cov2. A few cases of adults with COVID-19 and predominantly antibody deficiencies have been reported3,4; some of them developed acute respiratory distress syndrome (ARDS), while some had a milder course of illness. Based on what we know, innate immune defects in genes involved in type 1 interferon response (such as IRF7, IRF9, TLR3) are the most likely candidates to result in severe disease and death in patients with flu-like virus infection5. In a few cases of fatal influenza A (H1N1), variants in genes associated with familial hemophagocytic lymphohistiocytosis (FHL) and a decreased cytolytic function of NK cells, were also reported6.Our patient was on monthly supplemental IVIG treatment, and he received an additional dose during his hospital stay. This, and his young age, might have ameliorated the clinical course7. He had a favorable evolution, despite the known susceptibility to viral infection and immune dysregulation in ARPC1B deficient patients1. There were no signs of severe infection, ARDS, hyperinflammation or of “cytokine storm” unleashed by SARS-CoV-2. Despite his having a combined immune deficiency, our patient fully recovered without the need of additional supportive measures other than IVIG, supplemental oxygen and antibiotic treatment directed against the documented bacteremia.Although pediatric cases of COVID-19 are fewer compared to adults, some severe presentations and deaths among children have been reported. The presence of a restricted repertoire of IgG (since infants have no previous exposure to coronaviruses) might play a role in the better outcome seen in pediatric patients. Antibody-dependent enhancement has been implicated in the development of severe COVID-19 in the elderly8. Additionally, lung cells from children and women show a lower expression of membrane-bound ACE-2, which may also be protective against severe pneumonia.Conceivably, some immune defects could protect patients with certain IEIs from mounting a full uncontrolled inflammatory response against SARS-Cov2. The cytoskeleton is a regulator of gene transcription, coupling cell mechanics with the activity of NF-κB. Coronaviruses are thought to alter the cytoskeleton architecture to facilitate viral replication and output9. Thus, ARPC1B deficiency and other actinopathies might limit SARS-CoV-2 replication. Furthermore, Th2 cytokines modulate ACE2 (angiotensin-converting enzyme 2) and TMPRSS2 expression in airway epithelial cells10, and children with allergies (asthma and/or allergic rhinitis) have a lower expression of ACE211. Patients with ARPC1B deficiency often have allergic diseases; their Th2-biased response could help explain the milder presentation seen in our patient. Insights from protective mechanisms in children, with and without certain immune defects, could facilitate the identification of therapeutic targets.Lina Maria Castano-Jaramillo1, MDMarco Antonio Yamazaki-Nakashimada1, MDSelma Cecilia Scheffler Mendoza1, MD, MSJuan Carlos Bustamante-Ogando2, MD, MSSara Elva Espinosa-Padilla2, MD, PhDSaul O. Lugo Reyes2, MD, MS.From the (1) Clinical Immunology Service, and the (2) Immunodeficiencies Research Unit, at the National Institute of Pediatrics, Mexico City, Mexico.Conflict of interests: NoneEthical statement: The patient and his family gave written informed consent for the diagnostic procedures and for publication of the case report.KEY WORDS: Primary immune deficiency, inborn errors of immunity, combined immune deficiency, ARPC1B deficiency, actinopathy, children, COVID-19, SARS-Cov-2, allergy, pneumonia, sepsis.