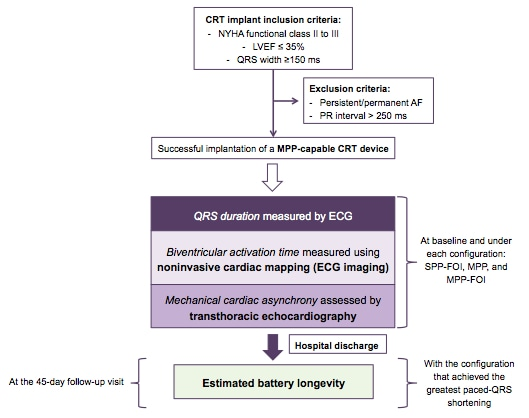
Background: Multipoint pacing (MPP) in cardiac resynchronization therapy (CRT) activates the left ventricle from two locations, thereby shortening the QRS duration and enabling better resynchronization; however, compared with conventional CRT, MPP reduces battery longevity. On the other hand, electrocardiogram-based optimization using the fusion-optimized intervals (FOI) method achieves more significant reverse remodeling than nominal CRT programming. Our study aimed to determine whether MPP could attain better resynchronization than single-point pacing (SPP) optimized by FOI. Methods: This prospective study included 32 consecutive patients who successfully received CRT devices with MPP capabilities. After implantation, the QRS duration was measured during intrinsic rhythm and with three pacing configurations: MPP, SPP-FOI, and MPP-FOI. In 14 patients, biventricular activation times (by electrocardiographic imaging, ECGI) were obtained during intrinsic rhythm and for each pacing configuration to validate the findings. Device battery longevity was estimated at the 45-day follow-up. Results: The SPP-FOI method achieved greater QRS shortening than MPP (-56±16 vs. -42±17 ms, P<0.001). Adding MPP to the best FOI programming did not result in further shortening (MPP-FOI: - 58±14 ms, P=0.69). Furthermore, the biventricular activation time according to ECGI was also shorter with SPP-FOI than with MPP. The estimated battery longevity was longer with SPP than with MPP (8.1±2.3 vs. 6.3±2.0 years, P=0.03). Conclusions: SPP optimized by FOI resulted in better resynchronization and longer battery duration than MPP.