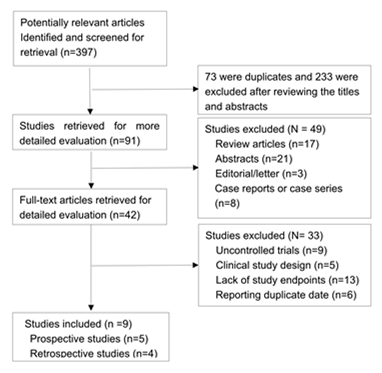
Background: Pulmonary veins reconnection due to insufficient lesions is an important cause of recurrence of atrial fibrillation (AF). High power ablation (HPA) with shorter duration or guided by Ablation index (AI) seen to increase efficacy and safety. This analysis aimed to evaluate the clinical benefits of HPA in patients with AF. Methods: The Medline, PubMed, Embase, and the Cochrane Library databases were searched for studies comparing HPA and conventional power ablation (CPA). Results: A total of nine trials with 2297 patients were included in the analysis. Pooled analyses demonstrated that HPA showed a benefit of first-pass pulmonary vein isolation (PVI) and acute PVs reconnection [risk ratio (RR): 1.27; 95% confidence interval (CI): 1.18–1.37, P < 0.001] and (RR: 0.52; 95% CI: 0.30–0.88, P = 0.01). HPA could reduce recurrence of atrial arrhythmias (RR: 0.71; 95% CI: 0.53–0.97, P = 0.03). Additionally, HPA was more beneficial in terms of procedural time [Weighted Mean Difference, (WMD): −41.19; 95% CI, −56.01 to −26.36, P < 0.001], ablation time (WMD: −19.45; 95% CI: −23.11 to −15.78, P < 0.001), and fluoroscopy time (WMD: −3.10; 95% CI: −5.52 to −0.68, P < 0.001) compared with the CPA approach. Moreover, HPA was associated with low complications (RR: 0.60; 95% CI: 0.36–0.99, P = 0.05). Conclusion: The HPA was a safe and effective approach for treating AF with clear advantages of procedural features. It was also associated with higher first-pass PVI, fewer acute PVs reconnection, recurrence of atrial arrhythmias and complications compared with the CPA approach.