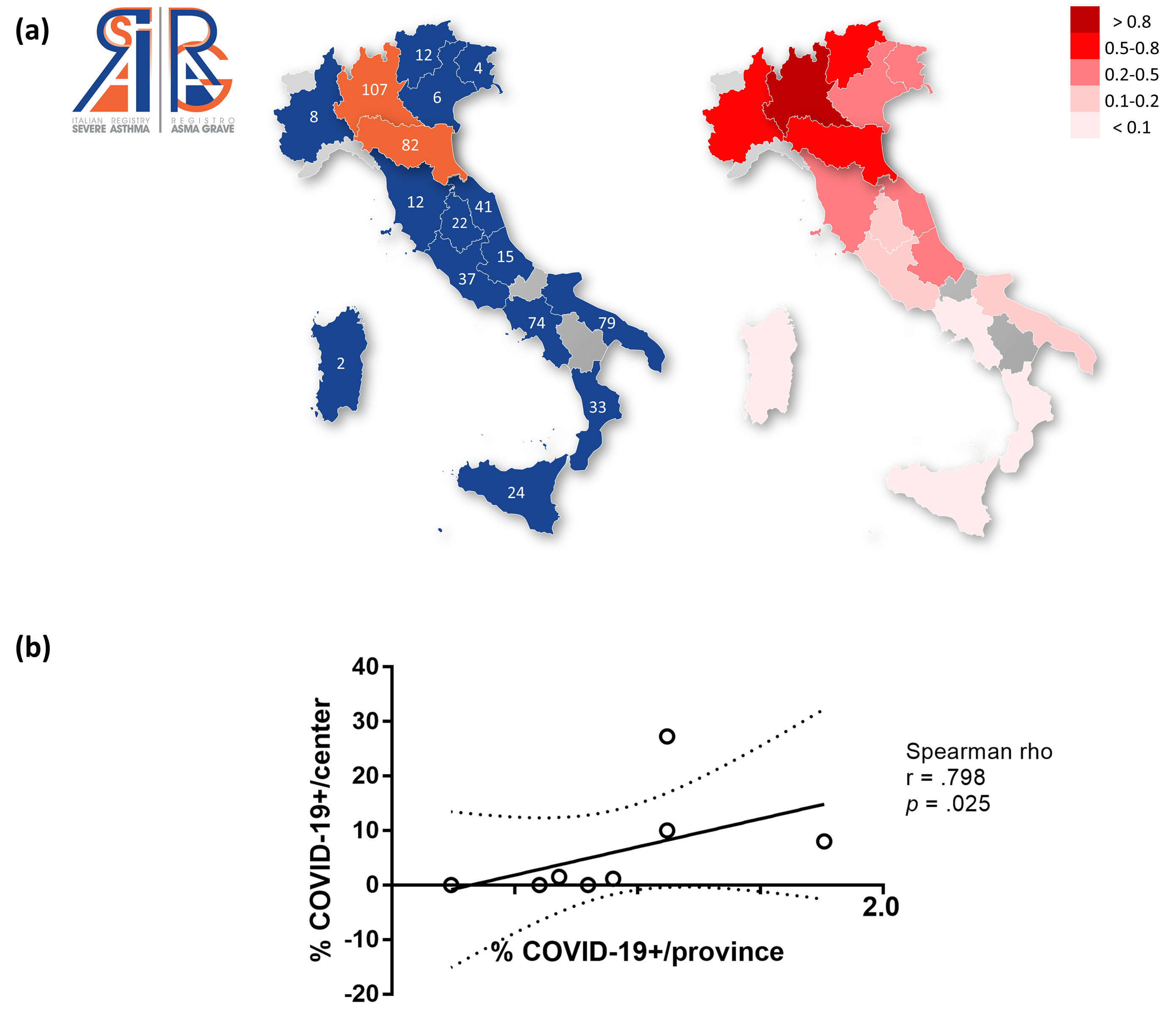
To the Editor, Severe asthma (SA) is a chronic disease affecting around 3-8% of adult asthma population in Europe, with the refractory form estimated to occur in 0.1% of the general population (1,2). SA is characterized by increased use of healthcare resources (i.e. emergency room/hospital admissions, access to intensive care units (ICU), use of biologics) due to exacerbations compared to the less severe form. In the current SARS-CoV-2 pandemic, there is an ongoing debate on the role of asthma and use of immunomodulating drugs, like corticosteroids and biologics, on COVID-19 outcomes. According to available data on COVID-19 hospitalizations, asthma seems to play little role on the clinical severity or access to health resources, unlike other chronic conditions such as hypertension, obesity and chronic obstructive pulmonary disease (3). However, to date, no information is available on the burden of SA on COVID-19 severity and hospitalization rates.A questionnaire was submitted to the Italian Registry of Severe Asthma (IRSA) network (4), assessing the prevalence and clinical characteristics of patients with SA who contracted COVID-19 during the outbreak in Italy (February 24th - May 18th 2020), and 41 out of 78 centers distributed evenly among different Italian regions participated to the survey (Figure 1a).Among the 558 subjects surveyed, 7 subjects contracted COVID-19 (1.25% of the national sample), with an average age of 54.5 years: 5 isolated at home/received home care (71.5%), while 2 subjects were admitted to the hospital (28.5%), none required accessed to ICU and no deaths were reported. All COVID-19 subjects with SA came from 2 regions of Northern Italy (6 Lombardy, 1 Emilia-Romagna, 3.7% of the regional population), all showing one or more comorbidities, and were treated with high-dose inhaled corticosteroids plus long-acting beta-2 agonists (ICS-LABA) and biologics (see Table 1).We then compared our results with data provided by the Italian Department for Civil Protection in the same time period from the affected geographic areas (5), and we observed that the frequency of COVID-19 among subjects referred to IRSA centers strongly correlated with the prevalence of SARS-CoV-2 infection in the corresponding province (Figure 1b). Furthermore, the hospitalization rate in COVID-19-SA subjects was not significantly different from the general population (24.1%, 23.6-24.6 95% C.I.; p=0.25, Chi-squared test). Lastly, we could not observe a significantly increased COVID-19 frequency in subjects undergoing high-dose ICS-LABA and biologics compared to SA treated with ICS-LABA alone (p=0.09, Fisher exact test).These findings from the IRSA registry offer some insights on the susceptibility to SARS-CoV-2 infection, access to healthcare resources and mortality by SA patients.Given the low prevalence of SA in Italy (2), we expected less COVID-19-SA cases per region than what reported by the IRSA survey. However, we observed that the geographic location of COVID-19-SA patients mostly reflected the bimodal distribution of the COVID-19 outbreak in Italy, mainly clustered in Lombardy and neighboring regions, where the highest cumulative COVID-19 cases were recorded (>500/100000 cases per inhabitants) (5). In these areas, the prevalence of positive cases by province also strongly correlated with the frequency of COVID-19-SA patients observed in each IRSA center (Figure 1b), suggesting that patients with SA most likely contract the infection when high circulation of the virus within the area of residence is present. The lack of positive cases reported in Southern regions further proves this hypothesis, and demonstrates the efficacy of the lockdown measures adopted to contain the further spread of the virus.Our results also suggest no increased risk of contracting COVID-19 in SA treated with biologics compared to ICS-LABA alone. Although there is currently no strong evidence that biologics used in asthma might affect the risk of contracting COVID-19, new evidence suggests a protective effect of inhaled corticosteroids against viral entry by ACE2 receptor downregulation, that are usually prescribed at a high dose in SA (6), thus a possible explanation to the lack of observed differences in our cohort.Despite the severity of asthma and reported comorbidities, no ICU admissions were reported, and hospital admissions in COVID-19-SA subjects did not differ from the median rate observed in the same geographic areas (5). Furthermore, we could observe no difference in the median monthly hospitalization rate of SA patients in 2019 compared to 2020 in Lombardy region where both hospital-admitted subjects reside (0.97 vs 0.9%, IRSA data).Our result is consistent with recent literature, showing that asthma in Western countries was not associated with an increased hospitalization rate and ICU admissions due to COVID-19 (3,8). It is still debated if a protective effect of Th2-inflammation in a significant proportion of asthma sufferers (7), or concomitant anti-inflammatory therapy could be the reasons for such outcomes (6). However, if asthma patients with COVID-19 require intubation, the duration of hospitalization was shown to be longer than average (8).As for the role of biologics in COVID-19 disease progression, we could not observe an increase in hospital admissions in patients with SA treated with biologics compared to the general population, with the majority isolating at home and requiring no additional treatment. Considering that, in areas with high prevalence of SARS-CoV-2 infection, 68.2% of SA subjects were treated with either omalizumab or mepolizumab, our observations further prove the safety of biologics during the COVID-19 pandemic.Lastly, we did not observe any deaths in our cohort, but we speculate that this outcome is most likely due to the small sample size and younger average age. In fact, advanced age seems to be the most determining risk factor on mortality due to COVID-19 compared to other causes. (9)Taken together, our results point at a neutral role of SA in the COVID-19 disease course and hospital admissions. One major strengths of our study is that, by using a fast and inexpensive tool, we could outline the salient features of severe asthma and COVID-19 at a national level, while the major weakness is the limited number of SA subjects diagnosed with COVID-19, that could lead to sampling bias and low accuracy. Further confirmation of these results with an increased sample size is therefore warranted