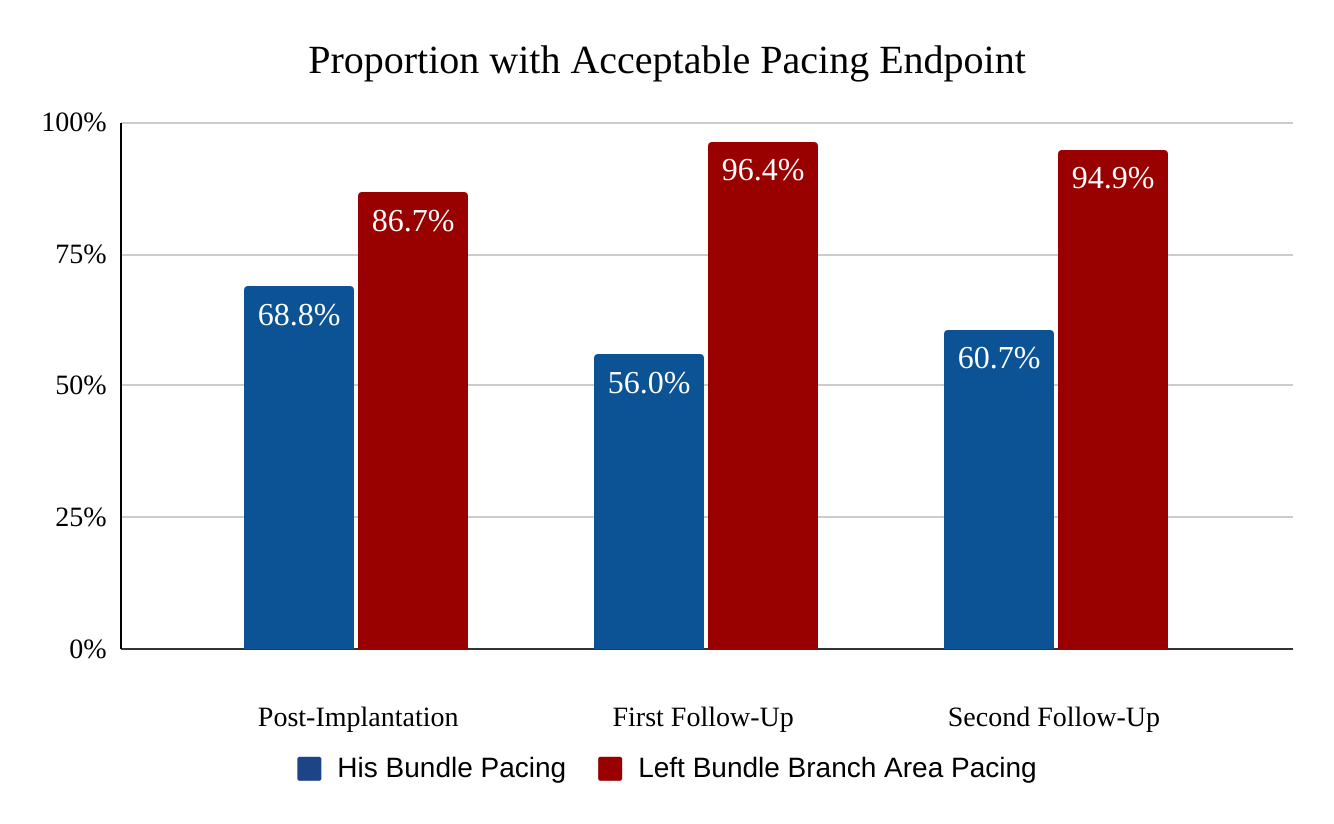
Background: Increasing interest in physiological pacing has been countered with challenges such as accurate lead deployment and increasing pacing thresholds with His-bundle pacing (HBP). More recently, left bundle branch area pacing (LBBAP) has emerged as an alternative approach to physiologic pacing. Objective: To compare procedural outcomes and pacing parameters at follow-up during initial adoption of HBP and LBBAP at a single center. Methods: Retrospective review, from September 2016 to January 2020, identified the first 50 patients each who underwent successful HBP or LBBAP. Pacing parameters were then assessed at first follow-up after implantation and after approximately one year, evaluating for acceptable pacing parameters defined as sensing R-wave amplitude >5 mV, threshold <2.5 V @ 0.5 ms and impedance between 400 and 1200 Ohms. Results: The HBP group was younger with lower ejection fraction compared to LBBP (73.2±15.3 vs 78.2±9.2 years, p=0.047; 51.0±15.9% vs 57.0±13.1%, p = 0.044). Post-procedural QRS widths were similarly narrow (119.8±21.2 vs. 116.7±15.2ms; p = 0.443) in both groups. Significantly fewer patients with HBP met the outcome for acceptable pacing parameters at initial follow-up (56.0% vs 96.4%, p = 0.001) and most recent follow-up (60.7% vs 94.9%, p = <0.001; at 399±259 vs. 228±124 days, p = <0.001). More HBP patients required lead revision due to early battery depletion (0 vs 13.3%, at an average of 664 days). Conclusion: During initial adoption, as compared with LBBAP, HBP is associated with a significantly higher frequency of unacceptable pacing parameters, energy consumption, and lead revisions.