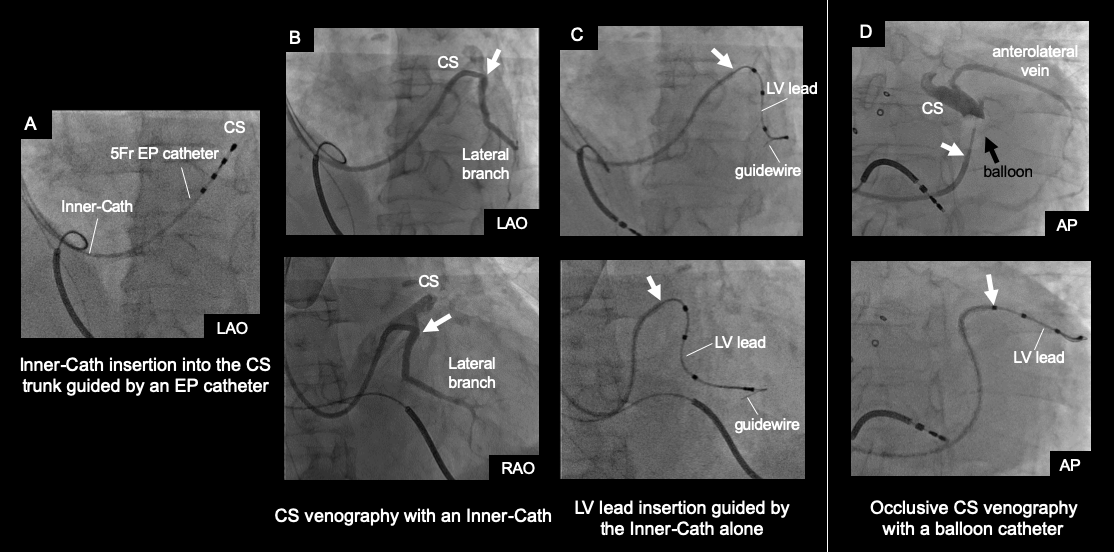
Introduction: Subselection inner catheters (Inner-Cath) are used adjunctively with outer guiding catheters (Outer-Cath) during cardiac resynchronization therapy (CRT) device implantation. This study aims to investigate the feasibility and efficacy of left ventricular lead placement (LV-LP) guided by Inner-Cath alone. Methods: A total of 74 patients undergoing de novo CRT implantation were investigated. LV-LP was initially guided by Inner-Cath in 42 patients (Inner-Cath group) and Outer-Cath in 32 patients (Outer-Cath group). In the Inner-Cath group, a 7Fr Inner-Cath was advanced to the coronary sinus through a 7 Fr sheath inserted in a subclavian vein. In the Outer-Cath group , 9Fr or 10Fr Outer-Caths were used. Success rate of LV-LP, additional use of inner or outer catheters and procedure-related complications were compared between groups. Results: LV-LP was successful in all patients in the Inner-Cath group while LV-LP had to be abandoned in 2 patients of the Outer-Cath group due to CS perforation caused by Outer-Cath manipulation. Procedure time was significantly shorter in the Inner-Cath group (148 vs 168 min; P=0.024). Deployment of both an inner and outer cath became necessary less frequently for the Inner-Cath group (4.8% vs 56.3%; P<0.001). Mechanical CS injuries due to guiding catheter manipulation were only observed in the Outer-Cath group (0% vs 15.6%, P=0.013). Conclusion: LV-LP guided by Inner-Cath alone was feasible in over 95% of the patients without severe complications. This methodology for LV-LP may be preferable in CRT candidates with severe LV dysfunction in terms of shorter procedure time, smaller guiding sheath and less complications.