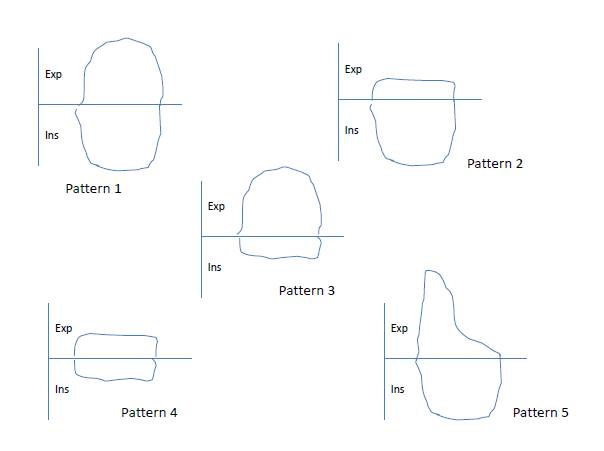
Introduction: For the diagnosis of airway anomalies, bronchoscopy is the gold standard. Infant pulmonary function testing is an emerging modality to assess airways and its utility in diagnosis and monitoring is unexplored in clinical studies. Objectives: To evaluate infant Pulmonary Function Test [Tidal Breathing Flow Volume Loop (TBFVL)] in children with airway anomalies and to correlate with bronchoscopy findings. Methods: We performed a prospective cohort study from July 2018 to April 2020 in children from 0-2 years with physician suspected airway anomalies. We performed TBFVL (graphic pattern and parameters) and bronchoscopy in these children and correlated the results. The primary outcome measure was a graphic pattern of TBFVL in children with laryngomalacia. Secondary outcome measures were bronchoscopy diagnosis of various airway anomalies, graphic pattern in children with airway anomalies other than laryngomalacia, measurement of TBFVL parameters and measurement of change in TBFVL graphic patterns and parameters at six months follow up. We compared TBFVL parameters with controls without airway anomalies. Results: We enrolled 53 children with both Infant Pulmonary Function Tests and bronchoscopy data. Isolated laryngomalacia (28, 52.8%) was the most common airway anomaly, followed by laryngo-tracheomalacia (7, 13.2%), laryngo-tracheo-bronchomalacia (6, 11.3%), and laryngomalacia with subglottic stenosis (4, 7.5%). Among isolated laryngomalacia, pattern 3 (fluttering of inspiratory limb) was most common in TBFVL, followed by pattern 4 (fluttering of inspiratory limb and flattening of expiratory limb) in 13 (46.4) and 8 (28.6%) cases, respectively. There was no strikingly predominant pattern in other groups of bronchoscopy diagnoses. Among TBFVL parameters, the ratio of Ti/Te was significantly high in children with isolated laryngomalacia compared to controls. Compared to controls, the tPTEF/tE was significantly higher in laryngomalacia plus sub-glottic stenosis. At six months of follow-up, clinical symptoms improved significantly, TBFVL pattern 1 (normal) became the most common pattern, and expiratory time increased significantly among TBFVL parameters. Conclusion: A particular type of airway anomaly may have a characteristic graphic pattern in TBFVL. Further, the TBFVL pattern may indicate improvement in the follow-up either spontaneously or after an intervention.