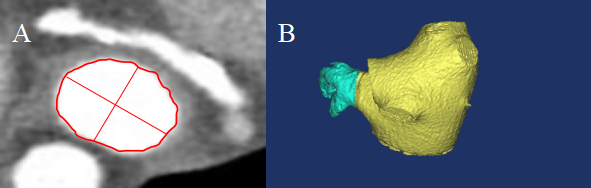
OBJECTIVES: To explore the value of detecting the peri-device leak (PDL) and device endothelialization after left atrial appendage closure (LAAC) by cardiac CT in patients with atrial fibrillation (AF), who underwent Watchman LAAC combined with radiofrequency ablation of atrial fibrillation (AFCA) METHODS: Patients with symptomatic drug-refractory atrial fibrillation at high risk of stroke (CHA2DS2-VASc Score ≥ 2), who underwent Watchman LAAC combined with AFCA in our center from March 2017 to December 2018 were enrolled Maximum diameter of LAA orifice was determined by preoperative CCTA A standardized view of Watchman device was obtained by postoperative CCTA multi-plannar reconstruction to evaluate the PDL and device endothelialization RESULTS: 84 patients post successful LAAC and AFCA were enrolled in this study Satisfactory LAA occlusion rate was 100% There were no death, bleeding, stroke, and device related thrombus (DRT) events At 6-month post procedure, CCTA images evidenced complete endothelialization in 44 patients (no contrast enhancement in LAA); contrast enhancement in LAA and visible PDL in 33 patients; contrast enhancement in LAA but without PDL in 7 patients (incomplete device endothelialization) Maximum diameter of LAA orifice could independently predict the occurrence of PDL (OR, 1.31; 95% CI, 1.11-1.55; P = 0.002), sensitivity was 69.7% and specificity was 80.4% with the cutoff value of maximum diameter of LAA orifice >28.2 mm on predicting PDL CONCLUSIONS: CCTA is feasible to evaluate PDL and device endothelialization after LAAC The maximum diameter of LAA orifice derived from CT can independently predict the occurrence of post-LAAC PDL