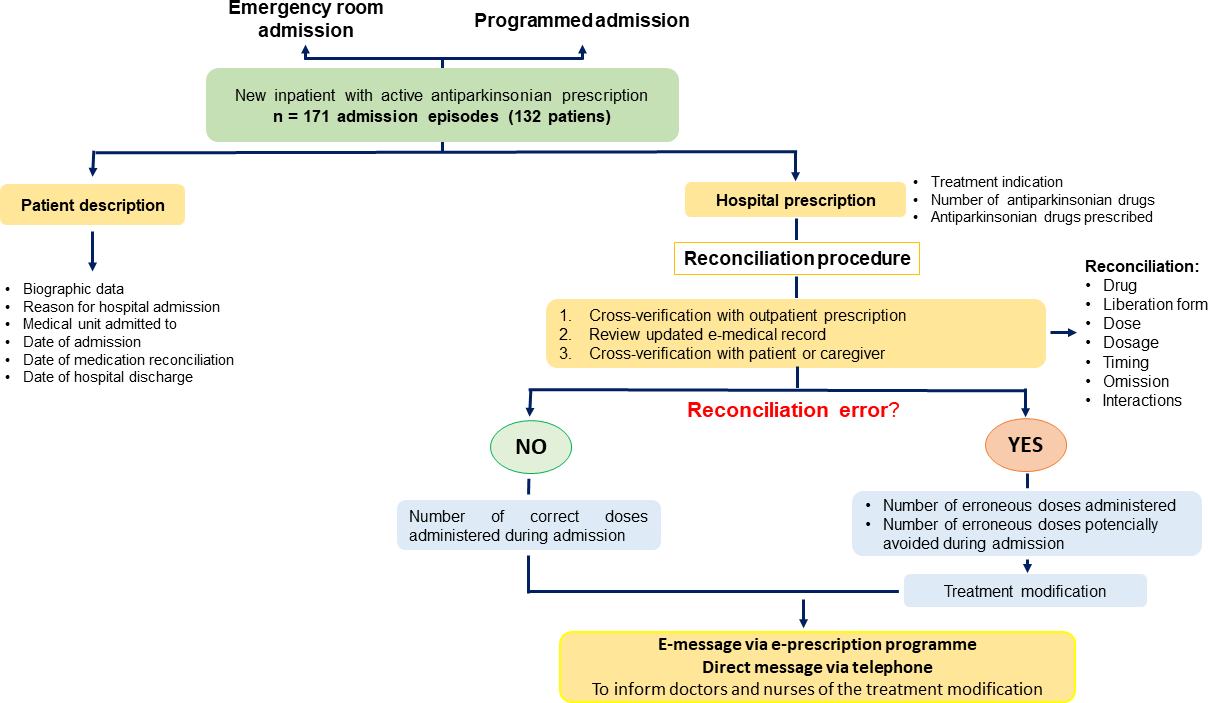
Pharmacotherapy is the primary treatment for this Parkinson’s disease, yet 70% of neurologists report that patients do not get their medication properly when hospitalized. The aim of this work was to implement a medication reconciliation protocol that allowed to identify and prevent antiparkinsonian medication errors to promote therapeutic quality and safety in daily practice. This was an interventional, single-center, one-year, prospective study. Medication reconciliation was performed using a three-phased check: inpatient electronic prescription validation after assessing the outpatient medication schedule, review of the latest Neurology report emitted by, and pharmacist-driven interview of the patient and/or caregiver. Of 224 prescription lines involving antiparkinsonian drugs, 179 contained, at least, one medication error (59.8%). Commission errors (91.62%) were more frequent than omitted drugs (8.38%). The most common medication errors were related to timing (41.90%), frequency (21.23%), and dosing (19.55%). Clinical pharmacists prevented the erroneous administration of 2716 antiparkinsonian doses, 60% of the total number of doses prescribed during this period, by performing this protocol. A significant relationship between the number of medication errors and the type of antiparkinsonian prescribed was evidenced (p<0.05). A contraindicated drug was prescribed in almost one-third of the episodes (29.82%), from these, 96% were changed after pharmacists’ recommendation.