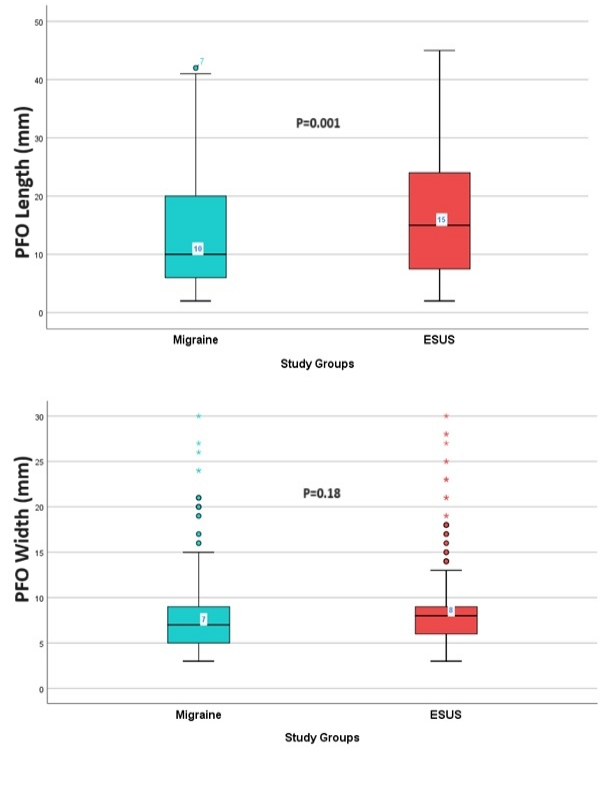
Background: This study aimed to compare patients with migraine and embolic stroke of undetermined source (ESUS) with known patent foramen ovale (PFO) in terms of echocardiographic and clinical features. Methods: In this observational single-center study, we obtained 2-dimensional (2D) and color Doppler images using parasternal short axis (PSAX), apical 4-chamber (A4C), and subcostal 4-chamber (SC4C) transthoracic echocardiography (TTE) views for patients with Migraine and ESUS. In cases where a PFO was suspected, patients underwent transthoracic contrast echocardiography and transesophageal echocardiography (TEE). We compared the anatomical and functional high-risk characteristics of PFO, as assessed by TEE and the RoPe score, in both patient groups. Results: This research involved a cohort of 720 individuals with ages ranging from 18 to 60, and 73.2% of the participants were female. Among the participants, 43.5% had Migraine, and 56.5% had ESUS. The most common comorbidity was diabetes (26.1%). PFO characteristics were measured, and high-velocity shunting through the interatrial septum was observed in 35.5% of patients. ESUS patients had a higher median age, with a similar gender distribution. ESUS patients had higher rates of diabetes and hypertension, while active smoking was more common in Migraine patients. Basic echocardiographic parameters were similar, except for higher pulmonary artery systolic pressure in ESUS. In the ESUS group, as compared to the migraine group, there was a more substantial occurrence of large microbubble passage through the interatrial septum, and the PFO showed increased length, while the PFO width remained similar. The RoPe and High-risk PFO scores were similar between the groups. Conclusions: ESUS patients were older with higher rates of diabetes and hypertension, while Migraine patients had a higher prevalence of active smoking. ESUS patients showed elevated pulmonary artery pressure, increased large microbubble crossings through the interatrial septum, and longer PFO lengths.

/Figure 1 (1).png?1698826372)